Canine thyroid carcinoma in 4-year-old American bulldog: Clinical pathology perspective
Dr. Lisa Viesselmann provides the clinical pathology perspective on this challenging oncology case.



Lisa Viesselmann, DVM
The goals of cytologic evaluation of canine thyroid tumors are to confirm the presence of thyroid neoplasia and to rule out other common causes of ventral cervical masses, including lymphadenopathy, sialoceles, cysts, abscesses and nonthyroid neoplasms. The thyroid gland may also be enlarged in the early stages of thyroiditis, prompting cytologic sampling. In these cases, lymphocytic inflammation may be diagnosed cytologically, but it is rare for dogs to be presented for veterinary evaluation in this acute phase of gland enlargement as other clinical signs of hypothyroidism are typically not yet present and enlargement is generally very mild.1 Cytologic samples of thyroid glands may be obtained via fine-needle aspiration or from impression smears of surgical biopsy samples. Since the normal location of the thyroid glands is in a highly vascular anatomic region, the use of a nonaspiration technique to sample a mass in this area may improve the cellularity of fine-needle samples by reducing the degree of blood contamination.1
Blood contamination is commonly a prominent feature of thyroid tumor aspirates, resulting in cytologic samples of variable cellularity. Thyroid follicular cells are fragile and tend to break easily during sample preparation. Consequently, thyroid tumors have a similar appearance to other endocrine and neuroendocrine neoplasms in that they are characterized by large numbers of free, round to oval nuclei in a sea of pale basophilic cytoplasm ("naked nuclei" morphology). Medullary thyroid cells (and to a lesser extent follicular cells) do tend to maintain some epithelial characteristics on cytology, often exfoliating in sheets or loose clusters, and sometimes forming acinar structures. However, the cytoplasmic borders within these clusters are often indistinct (Figure 2). Mild to moderate anisocytosis and anisokaryosis as well as occasional binucleation and prominent nucleoli may be seen, but the cells often lack striking features of malignancy except in poorly differentiated carcinomas.2 Therefore, cytologic appearance is not predictive of biologic behavior in these tumors.

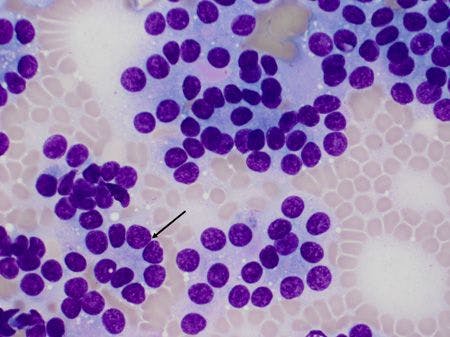
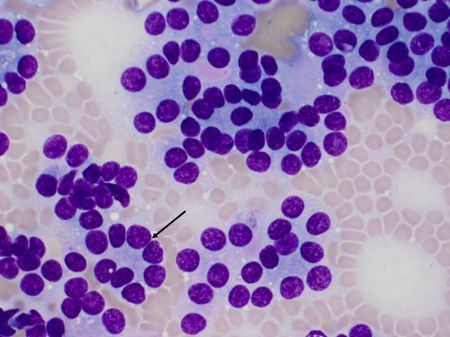
Figure 2. This image of a fine-needle aspirate from a canine thyroid carcinoma (500x magnification) demonstrates the loose clustering of cells with indistinct cytoplasmic borders that is typically seen with neuroendocrine neoplasms (not the patient in this case). The result is the appearance of naked nuclei embedded in a sea of free cytoplasm. A small acinar structure is also seen (arrow).
There are a few unique cytologic features of thyroid cells that can be useful in establishing their cellular origin. These features can be seen on aqueous and methanolic Wright's-stained samples, and while they do not aid in differentiating benign thyroid tissue from malignant neoplasia, they can be helpful in distinguishing cells of thyroid origin from cells of other endocrine or neuroendocrine neoplasms, such as carcinoid tumors, chemodectomas, apocrine gland anal sac adenocarcinomas and the pancreatic neuroendocrine tumors, which can all have a similar "naked nuclei" appearance cytologically. Most commonly, an extracellular amorphous eosinophilic material, thought to be colloid, will be present in association with cell clusters and occasionally in the center of an acinar arrangement of cells (Figure 3).

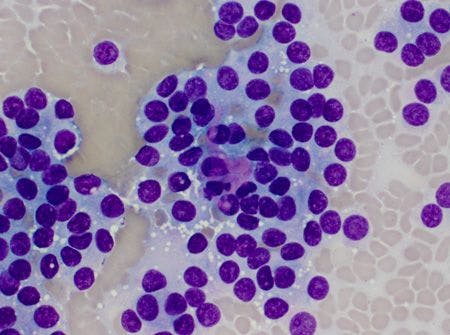
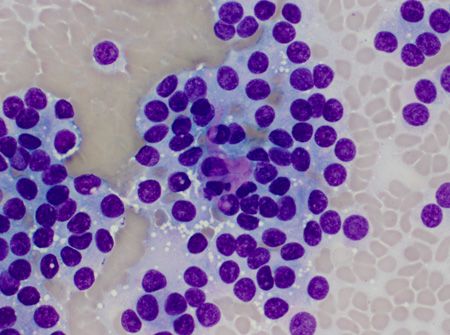
Figure 3. Amorphous, eosinophilic extracellular material (presumptively colloid) is present in association with a loose cluster of cells from a canine thyroid carcinoma (500x magnification) (not the patient in this case). This material is consistent with the thyroid origin of the cells and can be seen with both follicular and medullary thyroid cells.
In addition, a granular dark blue-black cytoplasmic pigment, thought to represent tyrosine, may be seen in intact follicular cells (Figure 4).

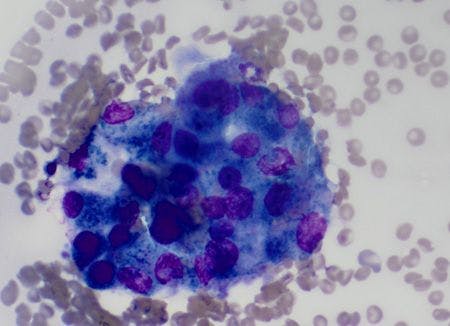
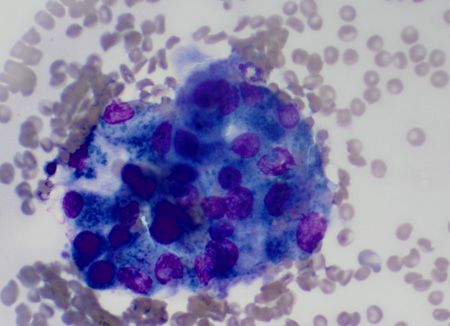
Figure 4. Numerous dark-blue cytoplasmic granules, thought to represent tyrosine, are seen within this cell cluster from a canine thyroid carcinoma (500x) (not the patient in this case). These granules are consistent with a follicular cell origin.
Both of these feautres are indicative of tissue of thyroid origin when they are seen, but their absence does not rule out the possibility of a thyroid mass. It is important to note that these features are seen in normal and hyperplastic thyroid tissue in addition to neoplastic cells.2 However, given that thyroid tissue in dogs can be present anywhere between the base of the tongue and the base of the heart, the presence of colloid or dark cytoplasmic granules on ctyology can aid in identifying the thyroid origin of an ectopic mass.3 It is also possible to see needle-like eosinophilic cytoplasmic inclusions in thyroid follicular cells (Figure 5). The composition and significance of these inclusions are unknown, and they can also be seen in cells from canine parathyroid carcinomas.1

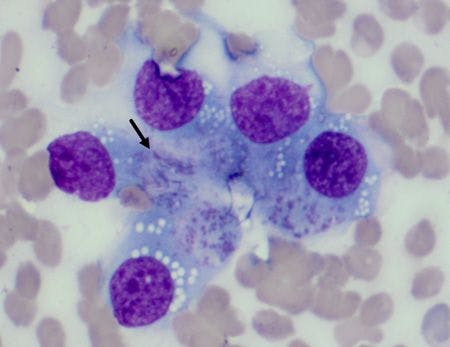
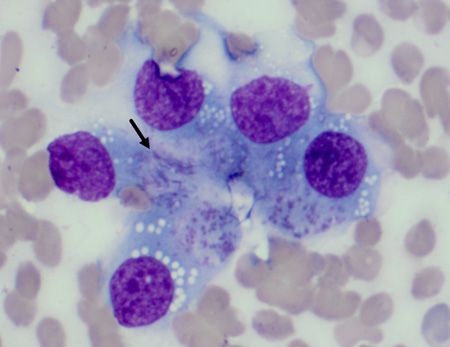
Figure 5. Needle-like eosinophilic inclusions (arrow) may be present within the cytoplasm of thyroid follicular cells (500x). The significance of these inclusions is unknown, and they are also frequently seen in canine parathyroid carcinomas.
Most palpable thyroid tumors in dogs are malignant, but they are typically interpreted cytologically simply as neuroendocrine tumors because of their characteristic naked nuclei morphology and because the relatively monomorphic appearance of the cells is not consistent with their biologic behavior. Additionally, in the absence of any identifying features of thyroid cells, it can be impossible to determine the tissue of origin based on cytology alone. Therefore, cytologic findings must be interpreted in light of the patient's history, clinical signs and imaging results, and definitive diagnosis and staging usually require histopathology with or without immunohistochemistry. Rarely, a thyroid carcinosarcoma will be present in a dog; this neoplasm is characterized cytologically by distinct epithelial and mesenchymal cell populations. This tumor tends to exhibit multiple striking features of malignancy, and histopathology with immunohistochemistry is required to differentiate between a carcinosarcoma and an anaplastic carcinoma.4
References
1. Valenciano AC, Cowell RL. Subcutaneous glandular tissue: mammary, salivary, thyroid, and parathyroid. In: Cowell and Tyler's diagnostic cytology and hematology of the dog and cat. 4th ed. St. Louis, Missouri: Elsevier;2014.
2. Raskin RE, Meyer DJ. Endocrine/neuroendocrine system. In: Canine and feline cytology, a color atlas and interpretation guide. 3rd ed. St. Louis, Missouri: Elsevier;2016.
3. Boes K, Messick J, Green H, et al. What is your diagnosis? Impression smear from an intracardiac mass in a dog. Vet Clin Pathol 2010;39:119-120.
4. Fernandez NJ, Clark EG, Larson VS. What is your diagnosis? Ventral neck mass in a dog. Vet Clin Pathol 2008;37:447-451.