Case report: A 5-year-old golden retriever with IDA
A look at the case management of a hunting dog with iron deficiency anemia secondary to chronic GI blood loss.
Sam, a 5-year-old 54.3-lb (24.7-kg) male golden retriever, was presented for evaluation of a four-week history of intermittent vomiting and anorexia, mild lethargy, and dark stools.
History
This hunting dog was adopted as a puppy. His initial growth was slower than his littermates' growth. When Sam was 1 year old, a jejunal resection and anastomosis was performed to correct a congenital stricture.
Physical examination and initial diagnostic tests
At presentation, Sam's temperature was 101.9 F (38.8 C), pulse was 100 beats/min, and respiratory rate was 24 breaths/min. His mucous membranes were pale pink and moist with a capillary refill time of < 2 sec. The rectal examination revealed soft stool that was slightly dark in color. Abnormal initial laboratory findings are listed in Table 1.



Table 1: Abnormal initial diagnostic test results
Additional diagnostic tests
No eggs, larvae, or trophozoites were found by using fecal sedimentation. The abdominal ultrasonographic examination revealed mild thickening of the gastric mucosal layer but no other significant findings. Sam's serum iron and ferritin concentrations were low, and total iron-binding capacity was increased (Table 2).

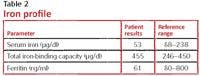
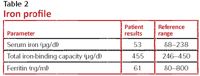
Table 2: Iron profile
A 250-ml packed RBC transfusion was administered, which raised the patient's packed cell volume to 33%. Gastroduodenoscopy was performed. No gross abnormalities were detected. Biopsy samples were collected from Sam's stomach and duodenum.
On exploratory laparotomy, Sam's organs appeared grossly normal. The site of the previous jejunal resection was identified. No lesions were noted on the serosal surface (Figure 1). This area was excised, and a new anastomosis was created. When opened, an area of ulcerated mucosa was evident (Figure 2).



1. Intraoperative serosal surface of the previous jejunal anastomosis. (Image courtesy of Dr. Kelley Thieman of Texas A&âs College of Veterinary Medicine and Biomedical Sciences.)
Histologic examination results of the gastric and duodenal specimens were unremarkable. Jejunum at the site of the previous anastomosis contained a focal mucosal ulceration and partial-thickness defect lined by inflamed granulation tissue and small blood vessels.



2. Mucosal surface of previous jejunal anastomosis. (Image courtesy of Dr. Kelley Thieman of Texas A&Mâs College of Veterinary Medicine and Biomedical Sciences.)
Outcome
Sam was treated with a single intramuscular injection of iron dextran (13 mg/kg) followed by two months of ferrous sulfate (250 mg orally once a day). Follow-up diagnostic test results showed a normal packed cell volume (43%), a normal mean corpuscular volume (68 fl), and an improved mean corpuscular hemoglobin concentration (36.6 g/dl).
Discussion
This case is an example of IDA secondary to chronic GI blood loss. Although the initial laboratory findings were highly suggestive of chronic hemorrhage and confirmed iron deficiency, the cause of the blood loss was not easily identified.
Minimally invasive diagnostic tests, including abdominal ultrasonography and gastroduodenoscopy, failed to identify the source of hemorrhage. This case highlights the role of an exploratory laparotomy in the work-up of chronic intestinal bleeding and the limitations inherent in examining only the serosal surface of the bowel.
The decision to resect the previous surgical site was appropriate and was made because no other abnormalities were evident. Although the underlying cause of the defect at the previous anastomosis is unknown, Sam did well after this surgical resection and iron supplementation.
















