A challenging case: Severe hypercalcemia in a puppy with hypoadrenocorticism
The point of interest in this case was not the disease, but the degree to which it caused an elevated calcium concentration.
A 5-month-old intact female English springer spaniel had been evaluated by the referring veterinarian for lethargy, decreased appetite, vomiting, and weight loss of one week's duration. A complete blood count (CBC) had revealed no abnormalities. Abnormal serum chemistry profile results were elevated blood urea nitrogen and creatinine concentrations, hypercalcemia, hyperphosphatemia, hyponatremia, and hyperkalemia (Table 1).

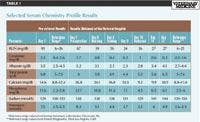

Table 1: Selected Serum Chemistry Profile Results
Treatment had included intravenous lactated Ringer's solution (26 ml/kg every 12 hours as a bolus) and injections of aminopentamide hydrogen sulfate (0.03 mg/kg every 12 hours), enrofloxacin (0.59 mg/kg every 12 hours—note that enrofloxacin is contraindicated in small- and medium-breed dogs between 2 and 8 months of age), and penicillin G (19,480 U/kg every 12 hours). The puppy's clinical signs had improved slightly after 24 hours of hospitalization, at which time it had been discharged to the owner. The referring veterinarian had tentatively diagnosed renal failure due to a genetic or congenital problem. A therapeutic renal diet had been the only treatment prescribed.
PHYSICAL EXAMINATION AND DIAGNOSTIC TESTING
Six days later (day 7), the puppy was referred to our hospital because of progression of clinical signs and for evaluation of possible renal failure. On presentation, the patient weighed 14.9 lb (6.8 kg) and was laterally recumbent and about 8% dehydrated. The puppy had a poor body condition, a dry and unkempt coat, bilateral mucopurulent ocular discharge, and waxy debris in both ears. The puppy's rectal temperature was 99.7 F (37.6 C), its heart rate was 150 beats/min, and its respiratory rate was 32 breaths/min. Its mucous membranes were pale-pink.



Vital Stats
We suspected hypoadrenocorticism and performed a CBC, a urinalysis, a serum chemistry profile, and an ACTH stimulation test. The CBC results revealed no abnormalities. The lack of a stress leukogram in this critically ill animal supported our suspicion of hypoadrenocorticism. The urinalysis results were normal, including a urine specific gravity of 1.020 (adult dog reference range = 1.015 to 1.050). Puppies older than 4 weeks of age have urine specific gravity measurements similar to those of healthy adult dogs.1 However, urine specific gravity is expected to be increased in the face of hypovolemic shock, even in a puppy.
Serum chemistry profile results revealed mild azotemia and hyponatremia and severe hyperkalemia, hypercalcemia, and hyperphosphatemia (Table 1, day 7). The sodium:potassium ratio in this puppy was 16.6. A sodium:potassium ratio < 24 is highly correlated with hypoadrenocorticism.2 We also considered primary hyperparathyroidism and secondary hyperparathyroidism due to renal failure as differential diagnoses for the hypercalcemia. However, because of the owner's financial limitations and our strong suspicion of hypoadrenocorticism, we did not measure ionized calcium and parathyroid hormone concentrations. Furthermore, the dog had been receiving a high-quality commercial puppy food and had no known ingestion of toxins such as rodenticides, psoriasis drugs, or excess vitamin D or calcium.
DIAGNOSIS AND TREATMENT
Initial treatment included a 400-ml bolus of 0.9% sodium chloride solution given intravenously over two hours (30 ml/kg/hr) followed by prednisolone sodium succinate (18.4 mg/kg IV), which was administered immediately after completion of an ACTH stimulation test. Intravenous fluid therapy with 0.9% sodium chloride solution was continued at 6.5 ml/kg/hr after the initial bolus. We administered cefazolin (30 mg/kg intravenously, two doses, 10 hours apart) and famotidine (0.75 mg/kg orally b.i.d. for the duration of hospitalization) to prevent sepsis due to bacterial translocation and ulceration secondary to compromised gastrointestinal mucosal integrity, which commonly occurs with hypoadrenocorticism.3
The ACTH stimulation test results were available the next day (day 8) and confirmed hypoadrenocorticism. The resting cortisol concentration was 0.5 µg/dl (reference range = 0.5 to 5.5 µg/dl), and the two-hour post-stimulation cortisol concentration was 0.4 µg/dl (reference range = 5.5 to 20 µg/dl). We treated the dog with a mineralocorticoid, desoxycorticosterone pivalate (Percorten—Novartis Animal Health; 2.2 mg/kg given intramuscularly), and glucocorticoids. Dexamethasone sodium phosphate (0.22 mg/kg intravenously) was administered once. The patient then began eating, so we switched to treatment with oral prednisone (1.5 mg/kg orally once a day).
Clinical signs resolved, and serum chemistry profile abnormalities, including the hypercalcemia, improved after three days of treatment for hypoadrenocorticism (Table 1, day 9). After four days of hospitalization, the patient was eating well and the ocular discharge had resolved, so the patient was released to the owner. Prednisone (0.73 mg/kg b.i.d.) and famotidine (0.73 mg/kg b.i.d.) were prescribed as initial home care. We emphasized the importance of strict compliance with future desoxycorticosterone pivalate injections and prednisone dosages.
At reevaluation (day 14), the patient was doing well. Its energy level and appetite had improved, and it had gained 1.3 lb (0.6 kg) since being released from hospital. Most serum chemistry profile results, including the calcium concentration, were normal (Table 1, day 14).
FOLLOW-UP
Initially, the patient was evaluated every 30 days, and more recently, it has been evaluated every 60 to 90 days. The results of intermittent serum chemistry profiles, including electrolytes, have been normal. Treatment includes desoxycorticosterone pivalate every four weeks, and the oral prednisone has slowly been tapered to a physiological dose of 0.3 mg/kg daily. We instructed the owner to increase the prednisone dose in times of stress, such as boarding or illness. The patient is a clinically normal 2.5-year-old dog.
DISCUSSION
Hypoadrenocorticism, or Addison's disease, is an endocrine disorder most commonly resulting from atrophy and destruction of the adrenal cortices. This deterioration leads to a deficiency of glucocorticoids alone or both glucocorticoids and mineralocorticoids.3,4
Many causes of this disease have been identified in people, including adrenal gland destruction (often autoimmune), tuberculosis, human immunodeficiency virus, adrenoleukodystrophy, and congenital adrenal hypoplasia.5,6 In dogs, primary hypoadrenocorticism is usually due to autoimmune destruction of the adrenal glands.3 Less common causes include granulomatous disease, infarction, neoplastic metastasis, amyloidosis, trauma, and iatrogenic causes.3 Natural secondary hypoadrenocorticism is due to a lack of ACTH production by the pituitary glands, which rarely occurs in dogs.3
Hypoadrenocorticism is most common in young to middle-aged female dogs, but it also occurs in neonatal and pediatric dogs.3,7,8 Standard poodles, West Highland white terriers, great Danes, Leonbergers, Labrador retrievers, and Portuguese water dogs are overrepresented breeds.3,8
The link between hypoadrenocorticism and hypercalcemia
Addison's disease may cause electrolyte abnormalities including mild to moderate hypercalcemia.9,10 Hypercalcemia is noted at the time of diagnosis in 29% of patients with hypoadrenocorticism.3 The severity of hypercalcemia in Addison's disease is typically proportional to the clinical severity of adrenal insufficiency.7,9 Although the exact mechanism of hypercalcemia associated with hypoadrenocorticism remains uncertain, the following theories have been postulated8,11,12 :
1. Dehydration leads to hemoconcentration and a relative increase in proteins that bind calcium.
2. Hyponatremia due to mineralocorticoid deficiency increases the affinity of plasma proteins for calcium. This increased protein binding of calcium leads to an elevated serum calcium concentration.
3. Decreased renal function and decreased glomerular filtration rate due to hypovolemia lead to increased tubular calcium reabsorption and decreased calcium excretion.
4. Increased serum calcium interferes with sodium and water retention in the distal renal tubules. A compensatory increase of sodium reabsorption then occurs in the proximal tubule, which is associated with an increase in calcium reabsorption.
5. Since glucocorticoids antagonize vitamin D activity, glucocorticoid deficiency, as with hypoadrenocorticism, can result in increased intestinal absorption and increased bone resorption of calcium. Glucocorticoids may alter osteoblast differentiation in a manner that has not been identified. Thus, a lack of glucocorticoids may cause an increase in calcium resorption from bone.
Many or all of these factors likely play a role in hypercalcemia associated with hypoadrenocorticism. The puppy in this report may have been at a higher risk to develop hypercalcemia because it had increased bone turnover due to growth.
The serum calcium concentration on presentation in the patient in this case was 26.8 mg/dl (reference range = 8.8 to 11.4 mg/dl), almost double that of previously reported concentrations of hypercalcemia associated with hypoadrenocorticism. Reported ranges of calcium concentrations in dogs with hypoadrenocorticism are 6.8 to 15.9 mg/dl (reference range = 8.5 to 11.5 mg/dl),7 12 to 14.9 mg/dl (reference range = 8.5 to 11.6 mg/dl),9 and—the highest reported value—16.7 mg/dl (reference range = 8.5 to 11.5 mg/dl).11
Hypercalcemia has toxic effects on all cell types, with clinically important effects on the heart and the nervous, gastrointestinal, and renal systems. Dogs with hypercalcemia commonly experience polyuria, polydipsia, anorexia, lethargy, and weakness.13 The development of these clinical signs depends on the severity and rate of development of hypercalcemia.13
Differential diagnoses for hypercalcemia
Hypercalcemia in dogs has many differential diagnoses other than hypoadrenocorticism, including primary hyperparathyroidism, acute and chronic renal failure, vitamin D toxicosis, nutritional secondary hyperparathyroidism, granulomatous diseases, neoplasia (e.g. carcinomas, lymphoma, multiple myeloma, melanoma), hyperthyroidism, and spurious laboratory results.14 Mild elevations in serum calcium concentrations (11 mg/dl) may occur in dogs up to 3 months of age because of normal bone growth.13 A small percentage of normal young dogs may have serum calcium concentrations as high as 12 mg/dl, possibly as high as 15 mg/dl.13 One published reference range for serum calcium concentrations in pediatric dogs is 10.6 to 11.7 mg/dl.15 No calcium or vitamin D supplements had been added to the high-quality commercial diet of the patient in this report.
Total serum calcium is the sum of ionized calcium (the biologically active form), protein-bound calcium, and complexed calcium. Spurious hypercalcemia can occur because of lipemia, hemolysis, dehydration, and acidosis and can also occur in young animals, postprandial samples, and samples containing EDTA anticoagulant.16 This puppy's calcium concentration was measured and verified at a commercial veterinary laboratory from a fasted, nonlipemic, nonhemolyzed sample that contained no anticoagulant. Dehydration may have increased the total serum calcium concentration in this patient. Ionized calcium concentrations help differentiate between spurious and true hypercalcemia. However, as previously stated, the financial limitations of the owners prevented this additional testing.
In this patient, primary hyperparathyroidism and secondary hyperparathyroidism due to renal failure were initially considered as differential diagnoses for hypercalcemia. Ideally, ionized calcium and parathyroid hormone concentrations would have been measured. However, because of the rapid, complete, and sustained resolution of hypercalcemia after treatment for hypoadrenocorticism, we thought no further testing was indicated.
Treating hypercalcemia
Hypercalcemia is best managed by treating the underlying cause. However, emergency measures to lower serum calcium concentrations are indicated while diagnostic test results are pending if the calcium-phosphorus product is
> 60.13 Saline diuresis promotes renal excretion of calcium. The additional filtered sodium competes with calcium for renal tubular reabsorption, so an increase in sodium results in enhanced calciuresis.14 After dehydration is corrected, furosemide is administered to inhibit calcium reabsorption in the thick ascending limb of the loop of Henle, which enhances calcium excretion.14 Furosemide was not required in this case because the hypercalcemia and hyperphosphatemia resolved in a few days with rehydration and treatment for Addison's disease. Glucocorticoids increase renal calcium excretion, decrease calcium resorption from bone, and decrease absorption of calcium from the intestinal tract. However, premature glucocorticoid administration may confound diagnostic test results for hypoadrenocorticism and lymphoma.14
Three forms of glucocorticoids were administered in this puppy. Prednisolone sodium succinate, a rapidly acting injectable glucocorticoid with a short half-life, was initially used when the puppy was obtunded. The subsequent injectable dose was with dexamethasone sodium phosphate, a slower-onset and longer-acting glucocorticoid. Once the puppy was eating, oral prednisone was administered and injectable glucocorticoids were discontinued. Hydrocortisone, prednisone, and prednisolone cross-react in the cortisol assay, so these glucocorticoid preparations must not be given before the ACTH stimulation test is completed.17
Prognosis
The prognosis for hypercalcemia tends to correlate with its cause, severity, and especially the solubility product of serum calcium and phosphorus. If the underlying cause cannot be treated, the prognosis is poor. When the solubility product of serum calcium and phosphorus is > 60 in dogs, soft tissue mineralization may occur, which can quickly result in renal and cardiac damage.13
CONCLUSION
In an Addisonian patient, hypercalcemia is not in itself remarkable. What is remarkable in the patient reported here is both the severity of the hypercalcemia (26.8 mg/dl) and the calcium-phosphorus product (608) on presentation and the dramatic improvement with treatment for hypoadrenocorticism.
Teresa L. Goodson, DVM, DACVIM
Susan C. Randell, BVSc, DACVIM
Affiliated Veterinary Specialists
9905 S. U.S. Highway 17-92
Maitland, FL 32751
REFERENCES
1. Faulks RD, Lane IF. Qualitative urinalysis in puppies 0 to 24 weeks of age. J Am Anim Hosp Assoc 2003;39(4):369-378.
2. Adler JA, Drobatz KJ, Hess RS. Abnormalities of serum electrolyte concentrations in dogs with hypoadrenocorticism. J Vet Intern Med 2007;21(6):1168-1173.
3. Feldman BF, Nelson RW. Hypoadrenocorticism (Addison's disease). In: Canine and feline endocrinology and reproduction. 3rd ed. St. Louis, Mo: Saunders, 2004;394-439.
4. Lathan P, Tyler J. Canine hypoadrenocorticism: diagnosis and treatment. Compend Contin Educ Pract Vet 2005;27(2):121-132.
5. Simm PJ, McDonnell CM, Zacharin MR. Primary adrenal insufficiency in childhood and adolescence: advances in diagnosis and management. J Paediatr Child Health 2004;40(11):596-599.
6. Perry R, Kecha O, Paquette J, et al. Primary adrenal insufficiency in children: twenty years experience at the Sainte-Justine Hospital, Montreal. J Clin Endocrinol Metab 2005;90(6):3243-3250.
7. Peterson ME, Kintzer PP, Kass PH. Pretreatment clinical and laboratory findings in dogs with hypoadrenocorticism: 225 cases (1979-1993). J Am Vet Med Assoc 1996;208(1):85-91.
8. Lathan P, Tyler J. Canine hypoadrenocorticism: pathogenesis and clinical features. Compend Contin Educ Pract Vet 2005;27(2):110-120.
9. Peterson ME, Feinman JM. Hypercalcemia associated with hypoadrenocorticism in sixteen dogs. J Am Vet Med Assoc 1982;181(8):802-804.
10. Willard MD, Schall WD, McCaw DE, et al. Canine hypoadrenocorticism: report of 37 cases and review of 39 previously reported cases. J Am Vet Med Assoc 1982;180(1):59-62.
11. Walser M, Robinson BHB, Ducket JW Jr. The hypercalcemia of adrenal insufficiency. J Clin Invest 1963;42(4):456-465.
12. Smith SA, Freeman LC, Bagladi-Swanson M. Hypercalcemia due to iatrogenic secondary hypoadrenocorticism and diabetes mellitus in a cat. J Am Anim Hosp Assoc 2002;38(1):41-44.
13. Schenck PA, Chew DJ, Nagode LA, et al. Disorders of calcium: hypercalcemia and hypocalcemia. In: DiBartola SP, ed. Fluid therapy in small animal practice. 3rd ed. St. Louis, Mo: Saunders Elsevier, 2006;122-194.
14. Feldman BF, Nelson RW. Hypercalcemia and primary hyperparathyroidism. In: Canine and feline endocrinology and reproduction. 3rd ed. St. Louis, Mo: Saunders, 2004;660-715.
15. Miller E. Diagnostic studies and sample collection in neonatal dogs and cats. In: Bonagura JD, Kirk RW, eds. Kirk's current veterinary therapy XII small animal practice. Philadelphia, Pa: WB Saunders Co, 1995;26-30.
16. Feldman EC. Disorders of the parathyroid glands. In: Ettinger SJ, Feldman EC, eds. Textbook of veterinary internal medicine diseases of the dog and cat, Volume 2. St. Louis, Mo: Elsevier Saunders, 2000;1508-1535.
17. Kemppainen RJ, Behrend EN. CVT Update: interpretation of endocrine diagnostic test results for adrenal and thyroid disease. In: Bonagura JD, ed. Kirk's current veterinary therapy XIII small animal practice. Philadelphia, Pa: WB Saunders Co, 2000;321-324.










Sweet pee new remedy in feline diabetes
November 9th 2023A novel class of drugs normalizes blood glucose in type 2 diabetic cats by dumping sugar into urine rather than modulating glucose uptake in the tissues but patient selection and close monitoring are crucial to using them safely
Read More


