Clinical Exposures: A true dermoid cyst on a golden retriever's dorsal skull
The owner of this retriever first noticed the golf-ball-sized mass three days before presentation.
A 14-month-old castrated male golden retriever was presented to a referral practice for evaluation of a cystic mass on its dorsal skull, medial and slightly rostral to the left ear.
HISTORY
The owner noticed acute onset of the golf-ball-sized mass three days before presentation, with no known associated trauma. Radiographic examination of the skull and cytologic examination of a fine-needle aspirate of the mass were performed two days earlier by the regular veterinarian. The results revealed a cystic subcutaneous mass over the frontal aspect of the skull and nonspecific suppurative inflammation. Six months before this presentation, the patient had a suspected cyst partially removed from the same location. The removed cystic segment was submitted for histologic examination, revealing a suspected incompletely removed dermoid sinus cyst.
DIAGNOSIS
Physical examination revealed ptosis of the left superior eyelid. Intact menace, pupillary light, and retractor bulbi responses were noted. Anisocoria, enophthalmus, and third eyelid protrusion were not seen. A large 5- to 6-cm raised soft movable mass over the left frontal and temporal skull was noted, which was painful on palpation.



Figure 1. A T1-weighted MRI contrast axial image of the frontotemporal subcutaneous cystic mass. Note the cavitary cyst lesion and surrounding extensive subcutaneous enhancement.
Complete blood cell count and serum chemistry profile results were unremarkable. Because of the previous suspicion of a dermoid sinus cyst, magnetic resonance imaging (MRI) was performed to further delineate the extent of the cyst and assess for potential sinus tracts. The MRI revealed a large cavitary subcutaneous mass along the left dorsal aspect of head, inciting a marked inflammatory reaction in the surrounding subcutaneous tissues. No evidence of communication with the central nervous system was noted (Figures 1 & 2).

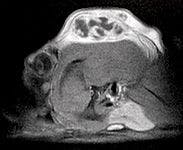
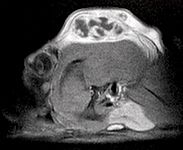
Figure 2. A T1-weighted MRI contrast sagittal image of the frontotemporal subcutaneous cystic mass. Note the cavitary cyst lesion and surrounding extensive subcutaneous enhancement.
TREATMENT AND OUTCOME
The cystic mass was surgically resected. An elliptical incision was made over the cystic mass site, removing soft and necrotic skin. A large area of multicavitary cystic tissue was encountered; most of this tissue was resected en bloc down to underlying temporal fascia. Within the center of this cystic, inflamed tissue, a small 0.5- to 1-cm white cyst containing long hair growth was noted (Figure 3). The cystic tissues were swabbed for culture. Once the affected tissues were removed, débridement of the remaining affected subcutaneous tissue was performed, followed by copious lavage. Two 1/4-in Penrose drains were placed in the resection defect. Subcutaneous and dermal closure was performed.



Figure 3. The resected cystic tissues, including an inner dermoid cyst with haired contents.
Postoperative analgesia (0.05 mg/kg hydromorphone every four to six hours), antibiotics (30 mg/kg cephalexin given orally every 12 hours), and crystalloid intravenous maintenance fluids were administered. The dog was discharged from the hospital the morning after surgery, and the drains were removed four days after surgery. Skin staples were removed 11 days after surgery, and the patient came in for rechecks one month and 13 months after surgery. The patient healed well from surgery and showed no sign of cyst recurrence.
HISTOLOGIC FINDINGS
Histologic assessment of the excised tissues revealed a dermoid sinus cyst with rupture and extensive chronic active dermatitis and panniculitis. Within the inflamed subcutaneous tissues, a cystic mass structure was noted, lined by well-differentiated basal and squamous epithelium with moderate hyperkeratosis. Subjacent to the cystic lining were numerous adnexal structures including follicles and apocrine glands.
DISCUSSION
Dermoid sinus cysts, also described as pilonidal sinuses or pilonidal cysts, are congenital defects stemming from incomplete neuroectodermal separation during embryogenesis.1-7 The condition is commonly seen in Rhodesian ridgebacks and is hereditary in the breed.8 Several reports have also described the condition in other breeds.2-3,9-13 These cysts are commonly reported to occur over the spine and less commonly in the nasal aspect of the dorsal midline.7,12 Other reported locations include the tongue, the parieto-occipital region, and inside the skull.14-16
Dermoid sinuses and cysts contain normal skin structures such as epidermis and adnexa.17 These factors differentiate the cyst in this report from infundibular or epidermal inclusion cysts, as the latter conditions do not have hair or adnexal structures. This patient's lesion was diagnosed as a dermoid sinus cyst partly because of its gross surgical appearance and the confirmatory findings of adnexal structures on histopathology.
Five types of dermoid sinuses have been described18 :
- Type I extends ventrally as a cylindrical sac.
- Type II has a saclike portion more superficial than type I.
- Type III has a superficial sac with no deep attachments.
- Type IV extends into and communicates with dura mater.
- Type V is a true cyst with a epithelial-lined sac.
The cyst in this report appears to be a type V dermoid sinus since it was a true cyst consisting of a closed, epithelial-lined sac. To our knowledge, the anatomic location of this unusual lesion has not been reported in the veterinary literature. In people, similar dermoid sinus cysts have been described in neonates and children.19 Some researchers have hypothesized that parasagittal dermoid sinuses on the head may occur along embryological fusion lines.16 In the context of this hypothesis, the lesion's location in this report may have originated from temporofrontal suture lines.
Dermoid sinus cysts are most effectively treated by complete surgical excision of involved tissues. Partial excision, as was initially performed in this patient, is likely to lead to recurrence of the clinical signs associated with the cystic lesion. Advanced imaging such as computed tomography or MRI are highly useful in assessing and delineating the lesion and any potential associated deep tracts.
Alon Kramer, DVM, DACVS
Department of Small Animal Surgery
Cornell University Veterinary Specialists
880 Canal St.
Stamford, CT 06902
Kei Hayashi, DVM, PhD, DACVS
Department of Surgical and Radiological Sciences
School of Veterinary Medicine
University of California
Davis, CA 95616
REFERENCES
1. Bellah JR. Surgical management of specific skin disorders. In: Slatter D, ed. Textbook of small animal surgery. 2nd ed. Philadelphia, Pa: Saunders, 1993;349-350.
2. Pratt JN, Knottenbelt CM, Welsh EM. Dermoid sinus at the lumbosacral junction in an English springer spaniel. J Small Anim Pract 2000;41(1):24-26.
3. Penrith ML, van Schouwenburg G. Dermoid sinus in a Boerboel bitch. J S Afr Vet Assoc 1994;65(2):38-39.
4. Marks S, Harari J, Dernell W. Dermoid sinus in a Rhodesian ridgeback. J Small Anim Pract 1993;34:356-358.
5. Scott DW, Miller WH, Griffin CE. Congenital and hereditary defects. In: Scott DW, Miller WH, Griffin CE, eds. Muller and Kirk's small animal dermatology. 6th ed. Philadelphia Pa; Saunders, 2000;936-937.
6. Walton-Angarano D, Swain SF. Congenital skin diseases. In: Bojrab MJ, Smeak DD, Bloomberd MS, eds. Disease mechanisms in small animal surgery. 2nd ed. Philadelphia Pa: Lea & Febiger, 1993;178-183.
7. Anderson DM, White RAS. Nasal dermoid sinus cysts in the dog. Vet Surg 2002;31(4):303-308.
8. Mann GE, Stratton J. Dermoid sinus in the Rhodesian Ridgeback. J Small Anim Pract 1966;7(10):631-642.
9. Selcer EA, Helman RG, Selcer RR. Dermoid sinus in a Shih Tzu and a Boxer. J Am Anim Hosp Assoc 1984;20:634-636.
10. Fatone G, Brunetti A, Lamagna F, et al. Dermoid sinus and spinal malformation in a Yorkshire terrier: diagnosis and follow-up. J Small Anim Pract 1995;36(4):178-180.
11. Cornegliani L, Ghibaudo G. Case report: a dermoid sinus in a Siberian Husky. Vet Dermatol 1999;10:47-49.
12. Bailey TR, Holmberg DL, Yager JA. Nasal dermoid sinus in an American cocker spaniel. Can Vet J 2001;42(3):213-215.
13. Cornegliani L, Jommi E, Vercelli A. Dermoid sinus in a golden retriever. J Small Anim Pract 2001;42(10):514-516.
14. Liptak JM, Canfield PJ, Hunt GB. Dermoid cyst in the tongue of a dog. Aust Vet J 2000;78(3):160-161.
15. Howard-Martin M, Bowles MH. Intracranial dermoid cyst in a dog. J Am Vet Med Assoc 1988;192(2):215-216.
16. Bornard N, Pin D, Carozzo C. Bilateral parieto-occipital dermoid sinuses in a Rottweiler. J Small Anim Pract 2007;48(2):107-110.
17. Gross TL, Ihrke PJ, Walder EJ. Veterinary dermatopathology: a macroscopic and microscopic evaluation of canine and feline skin disease. St. Louis, Mo: Mosby, 1992;351-372.
18. Miller L, Tobias K. Dermoid sinuses: description, diagnosis, and treatment. Compend Contin Educ Pract Vet 2003;25(4):295-300.
19. Denoyelle F, Ducroz V, Roger G, et al. Nasal dermoid sinus cysts in children. Laryngoscope 1997;107(6):795-800.










 in general practice")




