CVC Highlight: Alleviating cancer pain: A case study
Certain cases of cancer may respond well to conservative analgesic therapy initially but eventually require multimodal analgesia.
Editors' Note: This case was presented in a session entitled "Case studies in cancer pain management" during the International Veterinary Academy of Pain Management (IVAPM) symposium at CVC Kansas City, Aug. 30, 2009.
Tatou, a 9-year-old 92.4-lb (42-kg) neutered male Labrador retriever, was presented to the Hopital Veterinaire Rive-Sud oncology service for evaluation of a subcutaneous mass on the lateral aspect of the left antebrachium (Figure 1). The mass was associated with intermittent weight-bearing lameness that responded poorly to carprofen and tramadol; the latter caused anorexia, according to the owners.



Figure 1
Plain radiographs of the left forelimb demonstrated an aggressive mixed bone lesion in the ulnar diaphysis with osteolysis and some bone proliferation (Figure 2). Three-view thoracic radiographs obtained on the same visit did not show detectable pulmonary metastasis. Results of a complete blood count and serum chemistry profile and urinalysis were all normal except for an elevated alanine transaminase (ALT) activity (522 U/L; reference range = 10 to 100 U/L).



Figure 2
Fine-needle aspirates of the subcutaneous mass were obtained with a 22-ga needle and submitted for cytologic evaluation and staining for alkaline phosphatase (ALP) activity. A population of mesenchymal cells with small amounts of eosinophilic matrix consistent with osteoid was observed (Figure 3), and positive staining for ALP activity was demonstrated (Figure 4), suggesting a diagnosis of osteosarcoma.

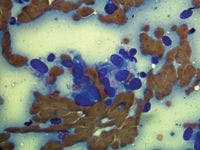
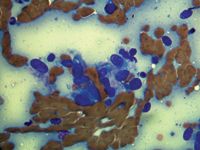
Figure 3
INITIAL TREATMENT
Because the tumor clearly extended in the extraosseous subcutaneous tissues of the antebrachium, an ulnectomy could not be recommended since complete surgical margins could not be obtained. Thus, the therapeutic options discussed included standard therapy combining amputation of the left forelimb and adjuvant chemotherapy as well as palliative options such as hypofractionated radiation therapy, intravenous aminobisphosphonate administration (pamidronate or zoledronate), and oral analgesic therapy.
The owners declined amputation and any injectable therapy. Because of the elevated ALT activity, they were instructed to discontinue carprofen administration, but they initially refused adjuvant analgesic therapy. Three weeks later, with the ALT activity back in the normal range, deracoxib was prescribed (1.2 mg/kg orally once a day). A good clinical response was observed with complete resolution of the lameness.
FOLLOW-UP CARE
Upon recheck visits over the next 12 months, Tatou was found to have an excellent quality of life and appeared perfectly comfortable with no evidence of detectable lameness or discomfort. The subcutaneous mass was noted to grow slowly over time. The results of periodic serum chemistry profiles were normal.
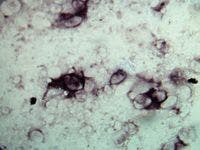
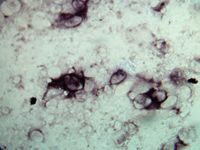
Figure 4
Thirteen months after diagnosis, the weight-bearing lameness recurred. A radiographic examination of the left forelimb showed progression of the bone lesion with more destruction and a larger soft tissue component. Thoracic radiographs then revealed advanced pulmonary metastatic lesions measuring up to 50 mm in diameter (Figure 5). The owners understood that the prognosis was guarded for survival but were instructed that additional analgesic therapy could be used to make Tatou more comfortable.



Figure 5
We opted to continue therapy with deracoxib because it was well-tolerated and provided adequate analgesia in monotherapy for more than a year and because the recurring pain and lameness were thought to be due to an increased level of pain rather than decreased analgesic efficacy of the drug itself. Tramadol hydrochloride was prescribed at a dosage of 4 mg/kg orally twice a day, as well as amantadine at a dosage of 5 mg/kg orally once a day.
Other palliative therapies were again discussed, such as radiation therapy or aminobisphosphonates (oral or injectable), but were declined. Nevertheless, Tatou responded well to the changes in medication, and the lameness again rapidly and completely resolved.



Figure 6
Tatou had an excellent quality of life for two additional months, but presented one day following an acute episode of nonweight-bearing lameness. A radiograph of the left forelimb confirmed a pathologic fracture of the ulna and the radius (Figure 6). The owners then opted for euthanasia, 445 days after diagnosis.
CONCLUSION
This case demonstrates that, though unusual, certain cases of cancer may respond well to conservative analgesic therapy initially but eventually require multimodal analgesia for proper control once pain progresses and becomes more severe. It also demonstrates that despite a poor prognosis once advanced metastasis is detected, palliative therapy to improve comfort should be considered and may result in added months of excellent quality of life.
Louis-Philippe de Lorimier, DVM, DACVIM (oncology)
Hôpital Vétérinaire Rive-Sud
7415 Boulevard Taschereau
Brossard (Québec) J4Y 1A2, Canada
















