Image Quiz: A Why is this 3-year-old pug acutely regurgitating?
Correct answer for Image Quiz: A Why is this 3-year-old pug acutely regurgitating?
Hiatal hernia is correct!
Although a diagnosis could not be made based on the survey radiographs (Figure 1A), a well-circumscribed region of contrast material is visible cranial to the diaphragm in the caudodorsal thorax up to 60 minutes after oral barium administration (Figure 1B). Note the focal narrowing of the contrast at the level of the diaphragm. These radiographic findings are consistent with a hiatal hernia.

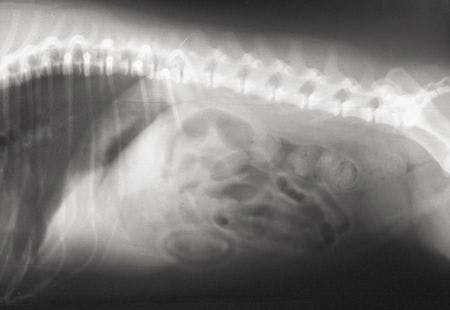
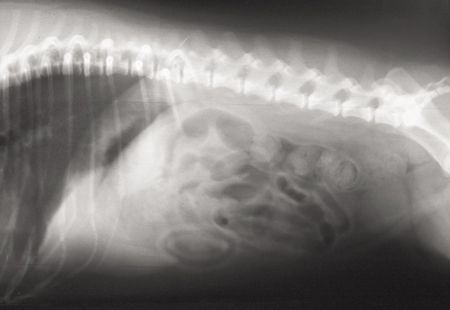
1A. A lateral radiograph of the caudal thorax and cranial abdomen in a 3-year-old spayed female pug with inspiratory stridor and a three-week history of regurgitation. The hiatal hernia is not visible.

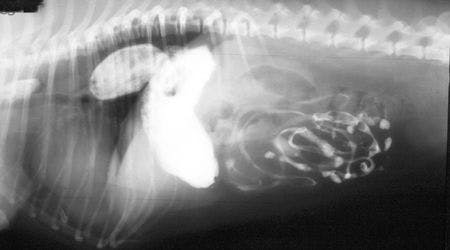
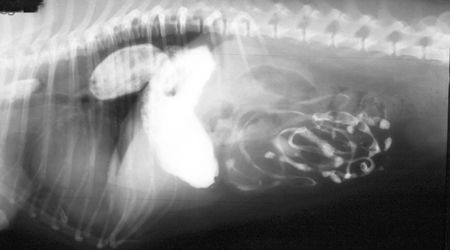
1B. A repeat radiograph taken 60 minutes after oral barium administration. Note the presence of the stomach cranial to the diaphragm.
Hiatal hernia classification
In dogs, hiatal hernias are relatively uncommon and can be classified into four different categories based on the structures involved.1
The most common type (and the type present in this case) is type I in which the abdominal esophagus, the gastroesophageal junction, and the cardia slide cranially through the esophageal hiatus into the mediastinum.1
In contrast, type II hiatal hernias involve movement of a portion of the stomach through the esophageal hiatus while the abdominal esophagus and the gastroesophageal junction remain in a normal position.
Type III hiatal hernias are a combination of both types I and II, and the term type IV is applied when other abdominal organs herniate in conjunction with either a type I or II hernia.
Which dogs are at risk?
Hiatal hernias are most often observed as congenital defects, especially in Chinese Shar-Peis and English bulldogs. In addition, trauma has been reported to cause hiatal herniation.2-4
Interestingly, in this case, while a congenital predisposition was suspected, the acute onset of clinical signs and the patient's age suggested an additional inciting factor. Increased inspiratory effort has been reported to cause hiatal hernias in predisposed dogs because of increased negative intrathoracic pressure, increasing the likelihood of abdominal organs passing through the esophageal hiatus. In this patient, the extra effort needed to overcome stenotic nares and an elongated soft palate was likely an important factor in the development of the hiatal hernia.1
Diagnosing a hiatal hernia
History, clinical signs, and a good physical examination will often guide diagnostics toward the upper gastrointestinal tract; however, imaging to visualize displacement of the abdominal esophagus and stomach will aid diagnosis in most patients.5
On survey radiographs, a hiatal hernia may be visible as a soft tissue mass in the caudodorsal thorax, generally to the left of midline.5,6 Gas is occasionally present within the mass, and evidence of aspiration pneumonia may be visible in the lung fields as a result of chronic regurgitation.3,6
Barium contrast studies may be necessary if survey radiographs are inconclusive.5 As in Figure 1B, contrast often persists cranially to the diaphragm with a constriction in the contrast column visible where the stomach passes through the esophageal hiatus.6 Occasionally, gastroesophageal reflux will be associated with a hiatal hernia, and chronic inflammation may be visible as a thickening of the esophageal wall cranial to the gastroesophageal sphincter.6
In many cases hiatal herniation is intermittent, and it may not be possible to image the stomach while it is cranial to the diaphragm if a single radiograph is taken.2,5 In such instances, it may be necessary to take multiple survey or contrast radiographs to visualize the hernia.6 Fluoroscopy has also been described as an adjunct to radiography to visualize the movement of the stomach and esophagus.2,5
Treatment and follow-up
Based on the radiographic findings, this patient underwent surgery for a hiatal hernia repair. The stomach was reduced back into the abdomen through the esophageal hiatus, and a hiatal plication, an esophagopexy, and a left-sided incisional gastropexy were performed to stabilize the stomach in the abdominal cavity and prevent recurrence (Figure 2). A staphylectomy and a wedge resection of the patient's nares were also performed to decrease inspiratory effort. The patient recovered uneventfully with complete resolution of clinical signs.

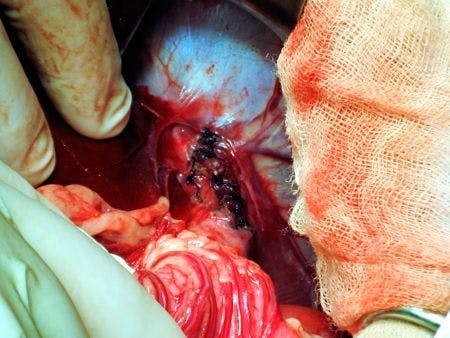
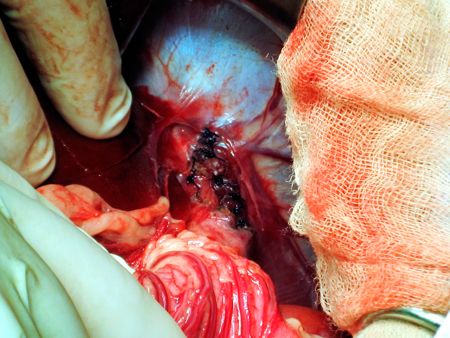
2. An intraoperative photograph showing the esophageal hiatus after plication and esophagopexy. The left liver lobes have been retracted to show the abdominal surface of the diaphragm.
REFERENCES
1. Sivacolundhu RK, Read RA, Marchevsky AM. Hiatal hernia controversies-a review of pathophysiology and treatment options. Aust Vet J 2002;80(1-2):48-53.
2. Bright RM, Sackman JE, DeNovo C, et al. Hiatal hernia in the dog and cat: a retrospective study of 16 cases. J Small Anim Pract 1990;31(5):244-250.
3. Gordon LC, Friend EJ, Hamilton MH. Hemorrhagic pleural effusion secondary to an unusual type III hiatal hernia in a 4-year-old great dane. J Am Anim Hosp Assoc 2010;46(5):336-340.
4. Guiot LP, Lansdowne JL, Rouppert P, et al. Hiatal hernia in the dog: a clinical report of four Chinese shar peis. J Am Anim Hosp Assoc 2008;44(6):335-341.
5. Lorinson D, Bright RM. Long-term outcome of medical and surgical treatment of hiatal hernias in dogs and cats: 27 cases (1978-1996). J Am Vet Med Assoc 1998;213(3):381-384.
6. Watrous BJ. Esophagus. In: Thrall DE, ed. Textbook of veterinary diagnostic radiology. 5th ed. St. Louis, Mo: Saunders Elsevier, 2007;495-511.
















