Immune-mediated hemolytic anemia: Treating cats and dogs with a complex disease
In cases of immune-mediated hemolytic anemia, flexibility in treatment protocols and anticipation of complications will help improve veterinary patient outcomes. Good client communication will help prepare owners for the rollercoaster ride that a diagnosis of IMHA in a pet can be.



Kristina / stock.adobe.comWhen immune-mediated hemolytic anemia (IMHA) is first identified, it is important for the veterinary team to plainly inform owners that the prognosis is variable and that the treatment can be labor-intensive, expensive and perhaps lifelong. Owners need to be prepared for the roller-coaster nature of this disease. And they need to be committed and on board for frequent recheck examinations. On the positive side, patients with the disease can have a good prognosis and relapse of IMHA is relatively uncommon.
In our companion article, “Immune-mediated hemolytic anemia: Understanding and diagnosing a complex disease,” we explored the pathophysiology and diagnosis of primary and secondary IMHA in dogs and cats. In this article, we will continue the discussion by reviewing the treatment options available and the factors that determine a prognosis for patients diagnosed with IMHA.
IMHA TREATMENT IN DOGS
Once a dog is diagnosed with IMHA, the decision to hospitalize the patient depends largely on the severity of clinical signs. If the disease is caught early and the patient is stable, close outpatient management is a reasonable option. More often, however, patients presenting with IMHA are already sick or unstable and need hospitalization for monitoring, supportive care and treatment.
The treatment of IMHA is extremely case-specific but generally involves the following principles:
- Limiting hemolysis with immunosuppressive therapy
- Treating tissue hypoxia
- Deterring the formation of thromboemboli
- Treating underlying conditions
- Providing supportive care
Limiting hemolysis with immunosuppressive therapy
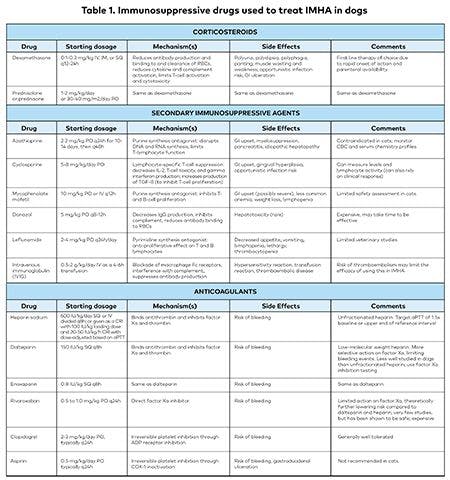
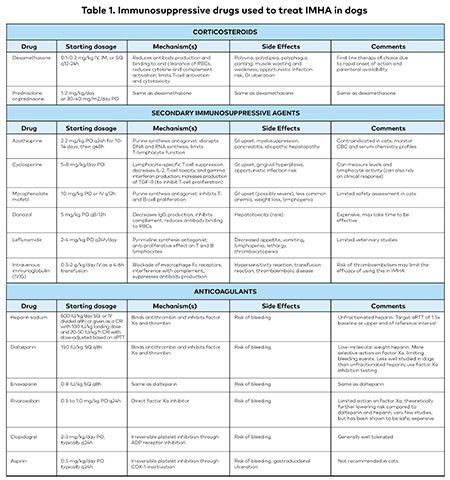
Numerous drugs have been described to treat IMHA (Table 1), but the first line of treatment is typically immunosuppressive corticosteroids. Secondary immunosuppressants are generally added early in the course of treatment to provide immunosuppression after tapering glucocorticoids, and they may also help with severe IMHA (very low hematocrit, severe autoagglutination, intravascular hemolysis or thrombocytopenia) or when the side effects of glucocorticoids become unacceptable. Even when IMHA might be secondary to infectious disease, you may need to administer immunosuppressive drugs to reduce the body's autoimmune response. However, they should be given with an appropriate antibiotic while you are awaiting infectious disease test results. In severe refractory cases, a tertiary agent may be used with caution. In such cases, though, you should be certain of the diagnosis because of the risk of opportunistic infection and other side effects.

Click for larger version.Even in the last decade, there have been numerous case reports describing opportunistic bacterial,1,2 protozoal3,4 and fungal infections,5-7 which demonstrate that any immunosuppressive drug carries risk. Therefore, we recommend careful monitoring of any patient that is immunosuppressed in an effort to treat IMHA.
Although immunosuppression is a cornerstone of therapy, head-to-head comparisons among different agents are uncommon, and the evidence to support one regimen over another is weak. Numerous factors including cost, frequency of drug administration, side effects and drug availability may determine which is appropriate for any given patient.
Corticosteroids. Dexamethasone SP (0.15 to 0.3 mg/kg, subcutaneously, intramuscularly, or intravenously, divided once or twice daily) can be given initially if oral medications cannot be tolerated. Prednisone or prednisolone (2 mg/kg per day, divided once or twice daily) is the oral drug of choice. Glucocorticoids are thought to prevent hemolysis by decreasing the clearance of antibody-coated red blood cells (RBCs) by macrophages, reducing the amount of antibody binding and complement activation on RBCs and, in the long-term, minimizing autoantibody production.8 Side effects include polyuria, polydipsia, polyphagia, increased panting, gastrointestinal ulceration, muscle wasting, fat deposition and increased susceptibility to infection. There are common changes in the serum chemistry, notably a cholestatic pattern of increased hepatic enzyme activity, but these do not indicate liver dysfunction and, as are the other side effects, they are reversible with steroid discontinuation.
Azathioprine. Azathioprine (2.2 mg/kg orally once daily for 10 to 14 days, then every other day) is frequently added as a second immunosuppressive agent because of its low cost, ready availability and limited adverse effects.9 Studies have shown increased survival times in dogs treated with glucocorticoids and azathioprine.10,11 The drawbacks to azathioprine are that it is only available in oral form and it can take weeks to take effect. Despite the increased survival times reported, a 2011 retrospective cohort study12 demonstrated no difference in 1-year survival between an azathioprine-prednisone combination and prednisone alone.
Azathioprine is a purine analogue antimetabolite that disrupts DNA and RNA synthesis and is effective in limiting cell-mediated immunity (T-lymphocyte function).13 Side effects are relatively uncommon and can include bone marrow suppression, pancreatitis and hepatotoxicity. Close observation for clinical signs, regular physical examinations and routine blood work will help to monitor for the more serious complications of this medication. Azathioprine can cause severe bone marrow and hepatic intoxication in cats, and its use is contraindicated.13
Rules of thumb for treating dogs and cats with IMHA
These guidelines should help you avoid some of the common mistakes that occur in managing IMHA.
Treat the treatable, especially if the therapy is unlikely to cause harm. We routinely start patients with IMHA on doxycycline while test results for infectious diseases are pending. Similarly, consider discontinuing any medications that are implicated in the onset of signs.
Taper drugs slowly. Cases are often referred to specialists when medications were tapered too quickly and patients relapse. For most cases of IMHA, while maintaining a secondary immunosuppressive agent at a constant dose, we typically reduce prednisone doses every 3 to 4 weeks, provided the packed cell volume is stable or improving. Immunosuppression with one or both agents should continue for a total of 4 to 6 months.
Be patient with bone marrow disease. If there is pure red cell aplasia or precursor-targeted immune-mediated anemia, a response to treatment may take more time than in cases of IMHA.
Anticipate therapy complications. Conduct routine screening for complications from medications, including CBC, biochemistry, and urinalysis and culture for opportunistic infections.
Treatment for Evans' syndrome and systemic lupus erythematosus (SLE) resembles that for IMHA. Distinguishing these diseases can be difficult, but the treatments are similar. If you are unsure whether a dog may have Evans syndrome (concurrent immune-mediated destruction of platelets) or SLE, treating the patient with immunosuppression may be a reasonable option. Do not give anticoagulant medications to patients with thrombocytopenia.
Consider referral for patients with very severe IMHA that require numerous transfusions, that are not responding to treatments as expected or that have atypical features of the disease. Some patients may need additional diagnostics that are not performed at all clinics, such as abdominal ultrasonography or bone marrow aspiration; or they may benefit from additional treatment options that are not typically available in general practice, such as therapeutic plasma exchange.
Don't confuse severe illness with a poor prognosis. Every animal is an individual. Even if all prognostic factors are poor, your patient may have a favorable outcome.
Cyclosporine. Cyclosporine (5 to 8 mg/kg orally twice daily) may also be used to treat IMHA. An intravenous form is available, but no clinical trials with this form have been published in the veterinary literature. The one retrospective study that investigated cyclosporine showed no benefit compared with other drug protocols.14
Cyclosporine is a potent T-cell suppressor that blocks production of immune-activating factors in both T-helper cells and T-cytotoxic cells, as well as blocking the expression of IL-2 and gamma-interferon. The outcome is a reduction of cell-mediated immunity and antibody production. Side effects include gastrointestinal upset (which may be ameliorated by freezing the capsules without any loss of efficacy15), dose-dependent gingival hyperplasia16 and increased susceptibility to infection. In addition to assessing a patient's clinical response, it may be useful to measure trough levels or preferably perform functional assays of lymphocyte suppression to evaluate the patient for potentially toxic doses.17
Cyclophosphamide. Cyclophosphamide has fallen out of favor since a randomized, controlled, prospective clinical trial published in 2003 showed no improved recovery or survival times in patients treated with cyclophosphamide and prednisone compared with prednisone alone.18 A number of other studies have also documented decreased survival in patients treated with cyclophosphamide.10,14
Mycophenolate mofetil. Like azathioprine, mycophenolate mofetil (10 mg/kg orally or intravenously twice daily) targets B and T lymphocytes by inhibiting an enzyme necessary for de novo purine biosynthesis.8 At therapeutic doses, mycophenolate is minimally myelosuppressive, but gastrointestinal side effects can be substantial in dogs (gastrointestinal hemorrhage, anorexia and diarrhea). To minimize these side effects, the dose can be lowered to well-tolerated levels when used in conjunction with other myelosuppressive drugs.8 Two recent studies in dogs with IMHA, one with five dogs and the other with 30, have shown high rates of efficacy, with variable rates (16% to 100%) of gastrointestinal side effects.19,20 Oral mycophenolate is only available in 250-mg capsules and 500-mg tablets, but compounded forms are available.
Leflunomide. Leflunomide (2 to 4 mg/kg orally once daily), an inhibitor of pyrimidine biosynthesis, has been used to treat rheumatoid arthritis in people and granulomatous meningoencephalomyelitis, neoplasia, immune-mediated polyarthritis and graft rejection in dogs.8 There are anecdotal and limited, but favorable, reports about the use of this drug for treating IMHA. Side effects in dogs appear to be minimal and potentially dose-dependent but can include vomiting, diarrhea, lethargy, lymphopenia and anemia.21 The most recent case report of its use describes a dog with Evans' Syndrome that had a prolonged clinical remission with leflunomide and human intravenous immunoglobulin (IVIG) alone.22 A very recent retrospective study of 92 dogs showed a low rate of adverse events (12%) with a higher median dose in dogs with adverse events than those without. Although these authors describe equivalent efficacy and thus suggest a lower starting dose than previous studies, the efficacy of leflunomide as a sole agent could not be assessed in dogs with IMHA since these dogs all received concurrent therapies.21
Danazol. Danazol (5 mg/kg orally two to three times daily), a synthetic androgen, has been used to treat immune-mediated disease in people and is sometimes recommended in addition to standard therapies to treat IMHA in dogs. Danazol likely exerts its immunomodulatory effects by decreasing the production of IgG and cytokines, inhibiting complement activation and reducing the binding of antibody and complement to erythrocytes.13 Danazol is not widely used for three main reasons: it is expensive, it can take weeks to observe a clinical response and it is potentially hepatotoxic.9 While one study did not show an improved outcome with this drug, the small number of reports in the veterinary literature makes the utility of this drug difficult to assess.23
IVIG. Human IVIG (0.5 to 2 g/kg intravenously daily, given over 6 to 12 hours) has been used with increasing frequency to treat a variety of immune-mediated diseases in dogs, including IMHA. The mechanism of action of IVIG is thought to be a blockade of the Fc receptors on macrophages, thereby reducing phagocytosis of antibody-coated RBCs, interfering with complement and suppressing antibody production. In addition, IVIG inhibits erythrocyte phagocytosis by binding to canine monocytes and lymphocytes and possibly by an anti-idiotypic down-regulation of antibody production.24
IVIG is typically expensive, and it can be given to patients with IMHA as a single infusion or on two or three consecutive days.25 Although IVIG appears to impart short-term benefits (reflected by a rising packed cell volume and reticulocytosis) within days of infusion, long-term benefits were not seen. IVIG administered to healthy dogs resulted in hypercoagulability, as assessed by repeated coagulation panels.26 Because of this, its use may be limited in cases of IMHA, where managing the risk of thrombosis is a critical component of successful treatment. Furthermore, a blinded, placebo-controlled randomized trial showed no difference in survival or length of hospitalization in dogs receiving glucocorticoids and IVIG.27
Liposomal-encapsulated clodronate. Liposomal-encapsulated clodronate (dichloromethylene diphosphonate) was the focus of two studies, only one of which was completed.28,29 This medication is a bisphosphonate that, when incorporated into liposomes, is rapidly phagocytized by macrophages leading to apoptosis. Intravenous liposomal-encapsulated clodronate has been shown to significantly reduce the number of canine splenic macrophages and dendritic cells in vitro, thereby obstructing the clearance of antibody-coated RBCs. This reduction, in effect, slows the clearance of opsonized erythrocytes and allows time for the other immunosuppressive drugs to work.
In an initial study in 2006, intravenous infusion of liposomal-encapsulated clodronate in healthy dogs and in seven dogs with IMHA showed that the drug is rapid-acting and well-tolerated.28 However, no additional peer-reviewed articles on its use have been published since then. In the 2006 study, results were favorable, and dogs treated with liposomal-encapsulated clodronate in conjunction with prednisone, azathioprine and heparin demonstrated improved survival compared to historical disease-matched controls.
Splenectomy. Splenectomy may be considered in refractory cases of canine IMHA. The benefits arise from removing one source of B cells and splenic macrophages, the primary culprits in the removal of antibody-coated erythrocytes.13 An abstract from a clinical study in 2003 showed increased survival with splenectomy (58% vs. 37.5% in the control group), but the sample size was small.30 A more recent study in 10 dogs suggested improved outcomes following splenectomy characterized by a decreased need for transfusions following surgery. Nine of 10 dogs survived, and four of those nine dogs discontinued immunosuppression without relapse.31
Consider splenectomy only in patients that have not responded to immunosuppressive medications, that require high-dose and long-term medications to maintain a remission or that are experiencing severe side effects from medications. Because there is an increased risk of developing a number of infections after splenectomy, the surgery is not recommended for patients taking multiple immunosuppressive medications. In addition, before performing the surgery in a stable patient, you will want to be sure to have negative test results for infectious diseases or consider empiric treatment for such diseases first.9
Therapeutic plasma exchange. Therapeutic plasma exchange (TPE) or plasmapheresis has been gaining acceptance as a treatment for refractory or severe cases of IMHA. TPE was first demonstrated in a dog in 2009,32 but descriptions of outcomes are limited to anecdotal and rare case reports. In TPE, a dialysis unit is used to remove the patient's plasma-and with it, the cytokines, procoagulant factors, complement and immunoglobulin implicated in erythrocyte lysis. Fresh-frozen plasma is administered in exchange. TPE has also been used in an attempt to treat kernicterus (bilirubin-induced encephalopathy), which may occur in severe cases of IMHA.33 Availability of TPE treatment is limited primarily to academic institutions and a few large referral practices. The potential for reduced hospitalization time and need for packed RBC transfusions may make TPE more appealing as a first- or second-line therapy, but further research is necessary.33
New therapies. New therapies being developed include monoclonal antibody therapy, attempting to re-induce self-tolerance, selective depletion of B cells, recombinant IL-2 therapy to induce regulatory T-cell production or transfusion of regulatory T-cells.34
Treating tissue hypoxia
Because of anemic hypoxia, patients with IMHA often need oxygen-carrying fluids to support them until immunosuppression begins to control the disease process. For example, research has shown that subclinical cardiac myocyte damage (presumably from anemia) in dogs with IMHA resolved as the IMHA was treated.35,36 It is rarely adequate to administer oxygen alone in severe anemia since the hypoxia is typically the result of low hemoglobin in the blood rather than poor oxygenation. Oxygen may help if a patient's clinical signs are complicated by thromboembolism.
The criteria for transfusion are not rigid but may include the presence of autonomic responses to anemia (e.g. severe tachypnea, dyspnea, tachycardia, cold extremities, weakness, mental depression or a hematocrit under 15%). If a patient appears comfortable when resting in a cage but becomes agitated and clinically unstable during necessary procedures, a transfusion may be indicated before proceeding.
The choice of administering packed RBCs, whole blood, or synthetic hemoglobin can be controversial and is often institution-dependent. Ideally, only the necessary component should be given. Because transfusion reactions can occur in patients that have not had transfusions previously, cross-matching should be done before transfusion in all nonautoagglutinating patients. Cross-matching should also be done in any dog that has received a prior blood transfusion. Since autoagglutination may interfere with accurate blood typing and cross-matching, packed RBCs should only be administered from universal donors (DEA 1-7 negative blood; DEA 4 can be positive) in dogs with IMHA.37
The product Oxyglobin is no longer available in the United States, but it may be beneficial in cases in which cross-matching is not possible or compatible blood is not available. Reports of the effect of Oxyglobin on outcome are contradictory.14,38
Deterring thromboembolism
Thromboembolism is the most common cause of morbidity and mortality in patients with IMHA and has been demonstrated in up to 50% of dogs with IMHA on necropsy.9 Given that numerous studies have shown hypercoagulability as a common finding in IMHA patients, anticoagulation is quickly becoming the standard of care, even when hypercoagulability cannot be proven. There are numerous anticoagulants, including those affecting coagulation factors like low-molecular-weight heparin, unfractionated heparin, warfarin and anti-Xa inhibitors (e.g. rivaroxaban) and those affecting platelets like ultra-low-dose aspirin and clopidogrel.
Heparin and anti-Xa inhibitors. Although two studies in the early 2000s failed to document increased survival with the use of unfractionated heparin,10,39 more recent research showed that by adjusting the dose of heparin, patients had improved outcomes compared with the prior approach of using fixed doses.40 If used, unfractionated heparin should be adjusted to prolong the activated partial thromboplastin time (aPTT) to 1.5x baseline or to inhibit factor Xa to a target range of 0.35 to 0.7 U/mL.
The most recently published studies on anticoagulation in dogs with IMHA demonstrate the safety of rivaroxaban, a direct anti-Xa inhibitor,41 and enoxaparin, a low-molecular weight heparin.42 Low-molecular-weight heparin (150 to 200 U/kg subcutaneously every 6 to 8 hours) is thus an alternative to unfractionated heparin. Low-molecular-weight heparins have better subcutaneous bioavailability, more specifically inhibit factor Xa (compared to unfractionated heparin and its more global effects on hemostasis) and have a theoretical lower risk of hemorrhage. Measuring anti-Xa activity is necessary to monitor the anticoagulant effects of these drugs, as their effect on aPTT is not proportional to the anticoagulant effect. Notably, the study evaluating the use of rivaroxaban was underpowered to determine its relative efficacy compared to ultra-low-dose aspirin or clopidogrel.41 The cost of these medications may limit the practicality of their use. Published studies on the clinical use of rivaroxaban are limited to a total of 24 dogs, with a dose ranging from 0.5 to 1 mg/kg PO q24h being well tolerated in all dogs.43,44
Warfarin. Warfarin is rarely used in veterinary medicine because it has a narrow therapeutic index and its absorption varies widely with the patient's diet and other medications being administered. In our literature review, we found no clinical studies of the use of warfarin in patients with IMHA, alone or compared to other anticoagulants. For these reasons, we prefer other anticoagulant therapies.
Clopidogrel and aspirin. The use of ultra-low-dose aspirin (0.5 mg/kg orally once daily) in addition to immunosuppressive medications has shown clear promise in canine patients. The beneficial effects of aspirin are thought to be from vasodilation and modulation of platelet aggregation. One study in dogs treated with glucocorticoids and azathioprine compared the use of ultra-low-dose aspirin, unfractionated heparin and a combination of these two medications.39 The results demonstrated that the patients treated with aspirin had significantly longer survival times than the patients treated with unfractionated heparin alone. In this study, the use of aspirin was not associated with any adverse clinical effects, even when used with high-dose glucocorticoids. More recently, a 2011 paper showed similar short-term survival and no adverse effects in a comparison of ultra-low-dose aspirin therapy alone or in combination with clopidogrel, though because of a small sample size (eight dogs in each group) this study may not have been able to detect a small difference in outcome between the groups.45
Fresh-frozen plasma. Fresh-frozen plasma has also been used to prevent or treat hypercoagulability in dogs with IMHA. However, the one published study showed that the use of fresh-frozen plasma (10 mL/kg) with unfractionated heparin failed to prevent thromboembolic complications in IMHA patients.46 It is worth noting, though, that the dose of heparin in this study was substantially lower than recommended doses.
Treating underlying conditions
Timely recognition and treatment of an underlying disease can allow immunosuppressive drug therapy to be tapered more quickly. Antibiotic administration while awaiting confirmation of suspected infectious disease can improve the chances of recovery. Antibiotic choice should be tailored to suspected or endemic diseases with known association to IMHA. Thorough diagnostic testing can help detect underlying infectious or neoplastic causes of immune-mediated hemolysis, which, if missed, would make treatment unlikely to succeed. Finally, the quick detection of complications and the speedy removal of nonessential drugs that can cause an immune reaction can also improve the chances of survival.
Providing supportive care
Aggressive, detail-oriented supportive care is a critical factor for the successful treatment of IMHA. Good nursing care that includes daily intravenous catheter care, proper nutrition, short walks, low-stress handling and limited phlebotomy can also contribute to a better outcome. Peripheral intravenous catheter placement may be preferable to central placement of a catheter, which carries the risk of thrombosis.
Ancillary treatments and medications such as intravenous fluids, gastric protectants, promotility drugs and antinausea medications can all support a patient through the initial days of treatment. Intravenous fluids, especially in patients with intravascular hemolysis, may help prevent hemogloblin-induced nephritis. Removing unnecessary indwelling catheters may reduce the risks of thromboembolism.
LONG-TERM MANAGEMENT
A steady or rising hematocrit, increasing reticulocytes, decreasing spherocytes and resolution of autoagglutination (if present) indicate a positive response to therapy.9 Medication tapering should be tailored to the individual patient; it should not occur until the hematocrit has at least stabilized, if not normalized. We typically recommend that glucocorticoids be tapered by about 25% every 3 to 4 weeks. Anecdotally, many patients' hematocrits stagnate while on glucocorticoids and normalize after their cessation. If an underlying disease has been addressed or the response to treatment is rapid, drug tapering can occur more quickly. Measure the hematocrit five to seven days after discharge and again after each decrease in drug dosage. If relapse occurs, the glucocorticoid should be reinstituted at an immunosuppressive dose (2 mg/kg/day) and a (new) secondary immunomodulatory drug should be considered. Perform a complete blood count, reticulocyte count, blood smear, serum chemistry profile, urinalysis and urine culture every four to eight weeks as needed to monitor for drug side effects, infections and disease relapse.
We usually recommend 4 to 6 months of therapy in total. If a second immunosuppressive agent was started at the time of diagnosis, this often means glucocorticoids are stopped months before stopping the second agent. Although a study documented that about three months of therapy was sufficient in some dogs successfully treated for IMHA, a subset of dogs needed longer treatment, hence our recommendation for 4 to 6 months of therapy if treatments are well tolerated.47 After finishing all medications, rechecks should occur quarterly for a year, then biannually.
The link between vaccination and IMHA relapse is tenuous at best. However, many practitioners, out of precaution, advise against vaccinating patients in remission from IMHA. Refer to your state's veterinary practice act to determine which vaccinations are required by law, and then consider the benefits and risks of vaccination in any patient that has recovered from IMHA.
PROGNOSIS
Numerous studies evaluating prognostic factors in IMHA were summarized in a 2015 systematic review.48 Prognostic studies are generally poor in quality, and mixed results are common across studies. Two scoring systems (Tokyo and CHAOS) have been proposed to predict survival based on objective data (e.g. PCV, bilirubin), but the former was not robust when tested at another institution, and the latter has yet to be validated in a prospective manner.49,50 The prognostic factors most frequently associated with a poor outcome in cases of IMHA include hyperbilirubinemia and markers of reduced kidney function (BUN, creatinine).48 Many putative risk factors have not been evaluated in more than one study, or the studies have yielded conflicting results. Anecdotally, the presence of intravascular hemolysis also appears to impart a poorer prognosis.
Although the most common cause of death in IMHA cases is thromboembolic disease, dogs with a normal coagulability index (a thromboelastography measurement) were shown to have increased risk of death compared with those that were more hypercoagulable, suggesting disseminated intravascular coagulation in these patients.51 Similarly, thrombocytopenia may be protective.12 In one study in dogs with IMHA, there was no statistical difference in survival times in patients with or without baseline coagulation abnormalities.52
Relapse rates have been documented to be roughly 12% to 24%, although different protocols and studies make comparison difficult.10,47 If relapse occurs, reinstitute medications at immunosuppressive dosages and taper more slowly. The mortality associated with IMHA is documented to be between 29% and 70%, with a large percentage of deaths occurring within the first two weeks of diagnosis.47
CATS AND IMHA: TREATMENT AND PROGNOSIS
Because there are numerous potential causes for secondary IMHA in cats and treating an infectious condition with immunosuppression can have deleterious consequences, you should be cautious before initiating any therapy. That is, if you suspect IMHA in a cat based on its history, clinical signs and routine diagnostic test results, perform a feline leukemia virus (FeLV) test. Patients with FeLV infection often respond well initially to treatment but eventually succumb to the disease. Cats with Mycoplasma haemofelis infection typically have recurrent episodes of hemolytic anemia. These organisms can rarely be seen on a blood smear, so PCR testing is preferred. As you would with dogs, treat cats with an appropriate antibiotic (e.g. doxycycline 5 mg/kg PO q12h), immunosuppressive therapy and blood transfusions as needed.9
Cats with IMHA are initially started on immunosuppressive dosages of glucocorticoids. There is little information on the addition of secondary or tertiary immunosuppressive medications in cats with severe IMHA. Possible drugs to add include cyclosporine or cyclophosphamide.53 A case report of successful treatment with mycophenolate mofetil in two cats suggests this is a plausible treatment as well.54 Azathioprine, as noted above, is contraindicated in cats because of the risk of bone marrow and liver toxicosis. Studies have described the use of leflunomide in cats for other immune-mediated conditions, but none have evaluated its use in IMHA.55 We have successfully used splenectomy for rare cases of prolonged refractory hemolysis, but we do not use this routinely.
The prognosis in cats with IMHA is thought to be better than that of dogs, with an all-time mortality rate of 23.5% in one study, and a median survival time of close to 1.5 years in another.53,56 Differences in study modality prevent direct comparison, but these rates are lower than the reported 30% to 70% mortality rate in dogs. In one of these studies, cats with infectious anemia had statistically significant worse outcomes, further supporting the fair prognosis of primary IMHA.56 Potential prognostic factors for worse outcomes include hyperbilirubinemia and older age, whereas higher globulins and lymphocyte counts were associated with better outcomes.56
CONCLUSION
When IMHA is first identified, it is important to inform owners that the prognosis is variable, treatment is labor-intensive, hospitalization is expensive, treatment may require months or a lifetime and side effects from medications can be severe. Furthermore, since RBC counts and overall stability are often erratic in these patients, owners should be prepared for the rollercoaster nature of this disease. Owners also need to be prepared for frequent and sometimes costly recheck examinations. On the other hand, patients can have a good prognosis if they respond to treatment, tolerate the side effects of medications needed for treatment and do not succumb to secondary infections or thromboembolism. Relapse of IMHA is relatively uncommon. The identification and treatment of underlying disease, the advent of new immunosuppressive drugs and good supportive and owner care all contribute to increased survival in patients with IMHA.
Be sure to also read the companion article, “Immune-mediated hemolytic anemia: Understanding and diagnosing a complex disease,” in which we explore the pathophysiology and diagnosis of primary and secondary IMHA in dogs and cats.
References
1. Mohri T, Takashima K, Yamane T, et al. Purulent pericarditis in a dog administered immune-suppressing drugs. J Vet Med Sci 2009;71(5):669-672.
2. Foster JD, Hartmann FA, Moriello KA. A case of apparent canine erysipeloid associated with Erysipelothrix rhusiopathiae bacteraemia. Vet Dermatol 2012;23(6):528-e108.
3. Magaña A, Sánchez F, Villa K, et al. Systemic neosporosis in a dog treated for immune-mediated thrombocytopenia and hemolytic anemia. Vet Clin Pathol 2015;44(4):592-596.
4. Fry DR, McSporran KD, Ellis JT, et al. Protozoal hepatitis associated with immunosuppressive therapy in a dog. J Vet Intern Med 2009;23(2):366-368.
5. Armstrong PF, Sigler L, Sutton DA, et al. Fungal myelitis caused by Phialosimplexcaninus in an immunosuppressed dog. Med Mycol 2012;50(5):509-512.
6. Dedola C, Stuart APG, Ridyard AE, et al. Cutaneous Alternaria infectoria infection in a dog in association with therapeutic immunosuppression for the management of immune-mediated haemolytic anaemia. Vet Dermatol 2010;21(6):626-634.
7. Brown JS, Bennet PF, Labuc RH, et al. Lymphocutaneous infection with Scedosporium apiospermum in a dog on immunosuppressant therapy. Aust Vet Pract 2009;39(2):50-54.
8. Gregory CR. Immunosuppressive agents. In: Bonagura J, Twedt DC, eds. Current veterinary therapy XV. St. Louis: Elsevier Saunders, 2014;268-274.
9. Piek C. Immune-mediated hemolytic anemias and other regenerative anemias. In: Ettinger SJ, Feldman EC, Côté E, eds. Textbook of veterinary internal medicine. 8th ed. St. Louis: Elsevier, 2017;829-837.
10. Burgess K, Moore A, Rand W, et al. Treatment of immune-mediated hemolytic anemia in dogs with cyclophosphamide. J Vet Intern Med 2000;14(4):456-462.
11. Reimer ME, Troy GC, Warnick LD. Immune-mediated hemolytic anemia: 70 cases (1988-1996). J Am Anim Hosp Assoc 1999;35(5):384-391.
12. Piek CJ, van Spil WE, Junius G, et al. Lack of evidence of a beneficial effect of azathioprine in dogs treated with prednisolone for idiopathic immune-mediated hemolytic anemia: a retrospective cohort study. BMC Vet Res 2011;7(1):15.
13. McCullough S. Immune-mediated hemolytic anemia: Understanding the nemesis. Vet Clin North Am Small Anim Pract 2003;33(6):1295-1315.
14. Grundy SA, Barton C. Influence of drug treatment on survival of dogs with immune-mediated hemolytic anemia: 88 cases (1989-1999). J Am Vet Med Assoc 2001;218(4):543-546.
15. Bachtel JC, Pendergraft JS, Rosychuk RAW, et al. Comparison of the stability and pharmacokinetics in dogs of modified cyclosporin capsules stored at −20°C and room temperature. Vet Dermatol 2015;26(4):228-e50.
16. Namikawa K, Maruo T, Honda M, et al. Gingival overgrowth in a dog that received long-term cyclosporine for immune-mediated hemolytic anemia. Can Vet J 2012;53(1):67-70.
17. Morley P, Mathes M, Guth A, et al. Anti-erythrocyte antibodies and disease associations in anemic and nonanemic dogs. J Vet Intern Med 2008;22(4):886-892.
18. Mason N, Duval D, Shofer FS, et al. Cyclophosphamide exerts no beneficial effect over prednisone alone in the initial treatment of acute immune-mediated hemolytic anemia in dogs: a randomized controlled clinical trial. J Vet Intern Med 17(2):206-212.
19. Wang A, Smith JR, Creevy KE. Treatment of canine idiopathic immune-mediated haemolytic anaemia with mycophenolate mofetil and glucocorticoids: 30 cases (2007 to 2011). J Small Anim Pract 2013;54(8):399-404.
20. West LD, Hart JR. Treatment of idiopathic immune-mediated hemolytic anemia with mycophenolate mofetil in five dogs. J Vet Emerg Crit Care 2014;24(2):226-231.
21. Sato M, Veir JK, Legare M, et al. A retrospective study on the safety and efficacy of leflunomide in dogs. J Vet Intern Med 2017;1502-1507. https://doi.org/10.1111/jvim.14810
22. Bianco D, Hardy RM. Treatment of Evans' Syndrome with human intravenous immunoglobulin and leflunomide in a diabetic dog. J Am Anim Hosp Assoc 2009;45(3):147-150.
23. Miller E. The use of danazol in the therapy of immune-mediated disease of dogs. Semin Vet Med Surg (Small Anim) 1997;12(3):167-169.
24. Whitley NT, Day MJ. Immunomodulatory drugs and their application to the management of canine immune-mediated disease. J Small Anim Pract 2011;52(2):70-85.
25. White HL, O'Toole TE, Rozanski EA, et al. Intravenous immunoglobin studied as potential immune-mediated hemolytic anemia treatment. Vet Pract News 2003;15(2):31-34.
26. Tsuchiya R, Akutsu Y, Ikegami A, et al. Prothrombotic and inflammatory effects of intravenous administration of human immunoglobulin G in dogs. J Vet Intern Med 2009;23(6):1164-1169.
27. Whelan MF, O'Toole TE, Chan DL, et al. Use of human immunoglobulin in addition to glucocorticoids for the initial treatment of dogs with immune-mediated hemolytic anemia. J Vet Emerg Crit Care 2009;19(2):158-164.
28. Mathes M, Jordan M, Dow S. Evaluation of liposomal clodronate in experimental spontaneous autoimmune hemolytic anemia in dogs. Exp Hematol 2006;34(10):1393-1402.
29. Lunn KF. Liposomal clodronate as a novel treatment for immune-mediated hemolytic anemia in dogs. Clinical Trials and Research Projects, Colorado State University, Fort Collins, CO. Personal communication, October 2008.
30. Toll J, Arohnson M. Prospective evaluation of medical therapy with or without early splenectomy for treatment of severe immune-mediated hemolytic anemia in the dog, in Proceedings. Am Coll Vet Intern Med Forum, 2003.
31. Horgan JE, Roberts BK, Schermerhorn T. Splenectomy as an adjunctive treatment for dogs with immune-mediated hemolytic anemia: ten cases (2003-2006). J Vet Emerg Crit Care 2009;19(3):254-261.
32. Crump KL, Seshadri R. Use of therapeutic plasmapheresis in a case of canine immune-mediated hemolytic anemia. J Vet Emerg Crit Care 2009;19(4):375-380.
33. Tovar T, Deitschel S, Guenther C. The use of therapeutic plasma exchange to reduce serum bilirubin in a dog with kernicterus. J Vet Emerg Crit Care 2017;27(4):458-464.
34. Swann JW, Garden OA. Novel immunotherapies for immune-mediated haemolytic anaemia in dogs and people. Vet J 2016;207:13-19.
35. Gow DJ, Gow AG, Bell R, et al. Serum cardiac troponin I in dogs with primary immune-mediated haemolytic anaemia. J Small Anim Pract 2011;52(5):259-264.
36. Cartwright JA, Gow DJ, Gow AG, et al. Serum cardiac troponin I concentrations decrease following treatment of primary immune-mediated haemolytic anaemia. J Small Anim Pract 2015;56(8):516-520.
37. Johnson V, Dow S. Management of immune-mediated hemolytic anemia in dogs. In: Bonagura J, Twedt DC, eds. Current Veterinary Therapy XV. St. Louis: Elsevier Saunders, 2014;275-279.
38. Carr AP, Panciera DL, Kidd L. Prognostic factors for mortality and thromboembolism in canine immune-mediated hemolytic anemia: a retrospective study of 72 dogs. J Vet Intern Med 16(5):504-509.
39. Weinkle TK, Center SA, Randolph JF, et al. Evaluation of prognostic factors, survival rates, and treatment protocols for immune-mediated hemolytic anemia in dogs: 151 cases (1993-2002). J Am Vet Med Assoc 2005;226(11):1869-1880.
40. Helmond SE, Polzin DJ, Armstrong PJ, et al. Treatment of immune-mediated hemolytic anemia with individually adjusted heparin dosing in dogs. J Vet Intern Med 2010;24(3):597-605.
41. Morassi A, Bianco D, Park E, et al. Evaluation of the safety and tolerability of rivaroxaban in dogs with presumed primary immune-mediated hemolytic anemia. J Vet Emerg Crit Care 2016;26(4):488-494.
42. Panek CM, Nakamura RK, Bianco D. Use of enoxaparin in dogs with primary immune-mediated hemolytic anemia: 21 cases. J Vet Emerg Crit Care 2015;25(2):273-277.
43. Conversy B, Blais MC, Dunn M, et al. Anticoagulant activity of oral rivaroxaban in healthy dogs. Vet J 2017;223:5111. doi: 10.1016/j.tvjl.2017.03.006.
44. Morassi A, Bianco D, Park E, et al. Evaluation of the safety and tolerability of rivaroxaban in dogs with presumed primary immune-mediated hemolytic anemia. J Vet Emerg Crit Care 2016;26(4):488-494.
45. Mellett AM, Nakamura RK, Bianco D. A prospective study of clopidogrel therapy in dogs with primary immune-mediated hemolytic anemia. J Vet Intern Med 2011;25(1):71-75.
46. Thompson MF, Scott-Moncrieff JC, Brooks MB. Effect of a single plasma transfusion on thromboembolism in 13 dogs with primary immune-mediated hemolytic anemia. J Am Anim Hosp Assoc 2004;40(6):446-454.
47. Piek CJ, Junius G, Dekker A, et al. Idiopathic Immune-mediated hemolytic anemia: treatment outcome and prognostic factors in 149 Dogs. J Vet Intern Med 2008;22(2):366-373.
48. Swann JW, Skelly BJ. Systematic review of prognostic factors for mortality in dogs with immune-mediated hemolytic anemia. J Vet Intern Med 2015;29(1):7-13.
49. Goggs R, Dennis SG, Di Bella A, et al. Predicting outcome in dogs with primary immune-mediated hemolytic anemia: results of a multicenter case registry. J Vet Intern Med 2015;29:1603-1610.
50. Ishihara M, Fujino Y, Setoguchi A, et al. Evaluation of prognostic factors and establishment of a prognostic scoring system for canine primary immune-mediated hemolytic anemia. J Vet Med Sci. 2010;72:465-470.
51. Sinnott VB, Otto CM. Use of thromboelastography in dogs with immune-mediated hemolytic anemia: 39 cases (2000-2008). J Vet Emerg Crit Care 2009;19(5):484-488.
52. Scott-Moncrieff JC, Treadwell NG, McCullough SM, et al. Hemostatic abnormalities in dogs with primary immune-mediated hemolytic anemia. J Am Anim Hosp Assoc 2001;37(3):220-227.
53. Kohn B, Weingart C, Eckmann V, et al. Primary immune-mediated hemolytic anemia in 19 cats: diagnosis, therapy, and outcome (1998-2004). J Vet Intern Med. 2006;20(1):159-166.
54. Bacek LM, Macintire DK. Treatment of primary immune-mediated hemolytic anemia with mycophenolate mofetil in two cats. J Vet Emerg Crit Care 2011;21(1):45-49.
55. Lemetayer J, Taylor S. Inflammatory joint disease in cats: Diagnostic approach and treatment. J Feline Med Surg 2014;16(7):547-562.
56. Swann JW, Szladovits B, Glanemann B. Demographic characteristics, survival and prognostic factors for mortality in cats with primary immune-mediated hemolytic anemia. J Vet Intern Med 2016;30(1):147-156.
Dr. Zachary Kern is a small animal internal medicine resident at North Carolina State University. He arrived there by way of University of Pennsylvania School of Veterinary Medicine and internships at BluePearl Veterinary Partners in New York City and Veterinary Specialists and Emergency Services in Rochester, New York.
Dr. Karyn Harrell obtained her veterinary degree from Michigan State University, completed an internship at the University of Minnesota and a small animal internal medicine residency at North Carolina State University. After spending six years at the Animal Medical Center in New York City, she returned to North Carolina State University and is currently a clinical assistant professor.
















