The options for treating feline hyperthyroidism
The options for treating feline hyperthyroidism include surgery, medical therapy, and radioiodine therapy.
The options for treating feline hyperthyroidism include surgery, medical therapy, and radioiodine therapy. The choice among these options is based on the animal's clinical status (the severity of clinical signs and the presence of concurrent nonthyroidal illness), the costs, the clinician's experience, and the availability of radioiodine therapy.
TREATMENT OPTIONS
Surgery
Surgical removal of enlarged, autonomously functioning thyroid glands is frequently used to treat hyperthyroidism, especially when radioiodine therapy is not an option or a cat experiences side effects from long-term oral or topical medication. Assess affected cats carefully before surgery to detect concurrent medical conditions, such as renal or cardiac disease and hypertension. Since both thyroid glands are affected in more than 80% of hyperthyroid cats, bilateral thyroidectomy is usually necessary. Several thyroidectomy techniques have been developed to minimize the postoperative complications of bilateral thyroidectomy, such as hypocalcemia or recurrence of hyperthyroidism.
Damage to or removal of all four parathyroid glands during bilateral thyroidectomy results in hypocalcemia, the most common postoperative complication.1 To counteract this complication, researchers have evaluated the efficacy of autotransplanting parathyroid tissue in normal cats.2 They performed bilateral thyroidectomy and parathyroidectomy with parathyroid autotransplantation in eight healthy, random-source adult cats.2 They found that serum calcium concentrations normalized faster postoperatively than concentrations reported in cats undergoing bilateral thyroidectomy and parathyroidectomy. Parathyroid autotransplantation greatly reduced morbidity in cats that had undergone a parathyroidectomy. Autotransplantation should be considered in cats in which all four parathyroid glands have been removed or in cases in which the surgeon is concerned that accurate identification of all parathyroid tissue was not possible during bilateral thyroidectomy. The researchers also found that transplanted normal thyroid tissue was present in at least three of the eight cats. This indicates that, when performing autotransplantation in hyperthyroid cats, it is important to remove all associated thyroid tissue to prevent the recurrence of hyperthyroidism.
Some clinicians advocate sequential removal of bilaterally affected thyroid glands. Staging a bilateral thyroidectomy presumably allows time for ipsilateral parathyroid tissue to revascularize before the second thyroid gland is removed and the blood supply to the contralateral parathyroid glands is interrupted. However, little information has been published to show the long-term efficacy and safety of staged thyroidectomies.
Medical therapy
Medically treating hyperthyroidism involves the use of methimazole, carbimazole (a pro-drug to methimazole available outside of the United States), and iodine-containing agents such as ipodate, iopanoic acid, and iodate. These forms of medical therapy may be used alone or with b-blockers, such as propranolol hydrochloride.



Should you use transdermal methimazole in hyperthyroid cats?
Methimazole
Methimazole is currently the drug most commonly used to treat hyperthyroidism. It is effective as an oral drug but can also be administered transdermally (see boxed text titled "Should you use transdermal methimazole in hyperthyroid cats?"). Methimazole prevents iodine from being incorporated into the tyrosyl groups of thyroglobulin, the precursor of thyroid hormones. The medication may have side effects, including vomiting, self-excoriation, anorexia, hepatopathy, and hematologic abnormalities. The drug is given twice a day and is often used to normalize serum thyroid hormone concentrations before treating a cat with surgery or radioactive iodine. It appears that twice-a-day dosing is necessary because a recent report demonstrated that euthyroidism was restored in 87% of cats treated twice a day vs. 54% of cats treated once a day. No difference in the rate of gastrointestinal side effects or facial pruritus was noted between the two groups.3 See Table 1 for recommendations on diagnosing hyperthyroidism, laboratory testing, initiating methimazole therapy, and patient monitoring.


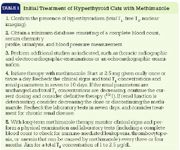
Initial Treatment of Hyperthyroid Cats with Methimazole
Carbimazole
An Australian study confirmed the efficacy and safety of carbimazole in the medical treatment of feline hyperthyroidism.4 The study included 25 cats in which hyperthyroidism was diagnosed during a 23-month period. Carbimazole therapy was instituted with owner consent, and rechecks were scheduled two, six, and 13 weeks after beginning therapy. The cats underwent a physical examination and hematologic and serum chemistry testing at each reexamination. Owners were also asked to assess clinical signs in the periods between rechecks. Fourteen cats treated with carbimazole responded favorably to therapy during the 13-week monitoring period. Side effects were minor and uncommon. Cats with underlying renal disease that became apparent during the study responded well to alterations in or cessation of carbimazole therapy.
Ipodate and iopanoic acid
Because 10% to 20% of cats treated with methimazole develop gastrointestinal side effects and carbimazole is not available in the United States, alternative medications are being studied. One study involved the use of ipodate, which is an iodine-containing contrast agent that inhibits the peripheral conversion of T4 to T3. This effect is similar to the effects of propranolol on thyroid function. In the study, 12 hyperthyroid cats were initially given oral ipodate at a dosage of 100 mg/day. The cats' clinical signs, body weight, heart rate, and serum T3 and T4 concentrations were evaluated two, four, six, 10, and 14 weeks after initiating ipodate.5 In addition, complete blood counts and serum chemistry profiles were performed at each recheck to detect any adverse effects. If a cat did not exhibit a good clinical response, the dosage of ipodate was increased to 150 mg/day and then to 200 mg/day at two-week intervals. Eight cats responded to the ipodate treatment, and four did not. Cats that responded exhibited mean body weight increases and mean heart rate and serum T3 concentration decreases during the study. Cats that did not respond exhibited mean body weight decreases and no significant changes in mean heart rate and serum T3 concentrations. Serum T4 concentrations remained high in all cats. None of the cats showed adverse clinical signs or hematologic abnormalities due to ipodate treatment. The study demonstrated that ipodate may be a feasible alternative to methimazole, particularly in cats that cannot tolerate methimazole and that are not candidates for surgery or radioiodine therapy. Cats with severe hyperthyroidism are less likely to respond to ipodate than are cats with mild or moderate disease. Also, in cats in which serum T3 concentrations do not return to the reference range, clinical signs are unlikely to improve adequately.
Since publication of the study, ipodate is no longer available in the United States. However, a similar product called iopanoic acid is available through compounding pharmacies. Like ipodate, iopanoic acid inhibits the peripheral conversion of T4 to T3. No published studies on the efficacy of iopanoic acid are available, but in my experience the dose, efficacy, and side effects appear to be similar to those reported with ipodate .
We do not know whether treatment with these iodine-containing contrast agents results in only temporary abatement of hyperthyroidism, as occurs in people, because no long-term studies have been done in cats. Animals that have been treated with ipodate or iopanoic acid probably should have the medication discontinued before beginning radioiodine therapy since both medications affect thyroid iodine uptake.
Potassium iodate and propranolol
In another recent study, researchers evaluated the use of a potassium iodate and propranolol combination in cats with hyperthyroidism before surgical treat ment.6 Potassium iodate appears to affect thyroid metabolism by blocking the uptake of iodine and leading, ultimately, to a drop in total T4 synthesis. Eleven cats (Group A) received propranolol on Days 1 through 10, followed by propranolol and potassium iodate on Days 11 through 20. These cats initially received 2.5 mg propranolol given orally every eight hours. If their heart rates exceeded 200 beats/min after four days, the dose was increased to 5 mg every eight hours. If the rates still exceeded 200 beats/min on Day 7, the dose was increased to 7.5 mg every eight hours. Ten cats (Group B) received only potassium iodate (42.5 mg orally t.i.d.) on Days 1 through 10, and then propranolol was added using the same treatment regimen as Group A. Surgery was performed on Day 21, and propranolol was continued for three days after surgery. The side effects of potassium iodate included intermittent anorexia, vomiting, and mild depression in some cats (i.e. seven cats in Group A; six cats in Group B). When this occurred, the dose was reduced to 21.25 mg every eight hours. Blood samples were obtained daily to measure concentrations of serum total T4, total T3, and reverse T3. The clinical signs improved in all cats during treatment. At surgery, 36% of the cats in Group A had normal serum total T4 concentrations, while 89% with initially elevated total T3 concentrations had normal concentrations. In Group B, 10% of the cats had normal serum total T4 concentrations, while 75% with initially elevated total T3 concentrations had normal concentrations. The drug regimen used in Group A was better-tolerated and more effective in normalizing thyroid hormone concentrations.
This potassium iodate and propranolol combination offers a medical alternative for those cats that cannot tolerate carbimazole or methimazole. All the cats in the study underwent thyroidectomy, so long-term medical control with this protocol was not studied. In addition, the use of iopanoic acid with propranolol should also be investigated because iopanoic acid appears to have fewer gastrointestinal and hepatic side effects than potassium iodate.
Radioiodine therapy
Radioiodine therapy appears to be the safest and most effective treatment for hyperthyroidism. Radioiodine can be administered intravenously, subcutaneously, or orally. While all routes appear effective, oral administration is discouraged because of the risks of exposure to people administering the medication and environmental contamination. The availability of radioiodine treatment has ex panded greatly in the past few years (Table 2). The cost of radioiodine treatment may initially seem prohibitive to pet owners, but advise them that long-term medical treatment or surgery will result in similar treatment costs.



Selected Radioiodine Facilities in the United States
The largest study of the safety and efficacy of radioiodine treatment involved 524 cats.7 A scoring system based on three factors (severity of clinical signs, size of the thyroid gland, and serum T4 concentration) was used to select the dose of radioiodine to be administered subcutaneously: 310 cats (59%) received a low dose of radioiodine (2.5 to 3.4 mCi; median = 3 mCi), 158 cats (30%) received a moderate dose (3.5 to 4.4 mCi; median =4 mCi), and 56 cats (11%) received a high dose (4.5 to 5.4 mCi; median = 5 mCi). Serum T4 concentrations were still increased in 80 cats (15.3%) when they were discharged from the hospital, but by six months after radioiodine administration, the serum T4 concentrations had dropped to within or below the reference range in all but eight cats (1.5%). Many cats had low serum T4 concentrations at some point after treatment, but only 11 cats (2.1%) developed clinical hypothyroidism and required L-thyroxine supplementation. Thirteen cats (2.5%) had a relapse of hyperthyroidism 1.1 to 6.5 years after the initial radioiodine treatment. The treatment response was good in 94.2% of the cats. Median survival time was two years; the percentage of cats alive after one, two, and three years of treatment was 89%, 72%, and 52%, respectively.


Selected Radioiodine Facilities in the United States (cont'd)
Cats with thyroid carcinoma are also candidates for radioiodine therapy, especially after surgical debulking. In one study, seven cats that had undergone surgical removal of thyroid carcinomas were treated with 30 mCi of radioactive iodine (131I).8 Six cats had clinical signs of hyperthyroidism. The 131I treatment caused no complications, and the cats' clinical signs resolved. Isotope uptake was not evident on four cats' technetium scans after treatment. In three cats, the isotope uptake was the same or less than the intensity of salivary gland uptake. Hypothyroidism occurred in all cats after treatment; four cats needed L-thyroxine supplementation. One cat was still alive 33 months after treatment. The other six cats were euthanized 10 to 41 months after treatment as a result of unrelated diseases.
Most doses of radioiodine are determined from experience, a combination of clinical and hormonal data (as above), or radioiodine uptake and thyroid volume in a given patient. A recent study evaluated the practicality and accuracy of using thyroid volume estimates in hyperthyroid cats to calculate the dose of radioiodine. For this study, hyperthyroidism was diagnosed in 80 cats with thyroid scintigraphy using technetium pertechnetate.9 Based on the volume of hyperfunctioning thyroid tissue indicated in the pertechnetate scans, a dose of radioiodine was calculated and administered to the cats. Several parameters were evaluated in an attempt to identify a difference between treatment success and failure. Cats that failed to become euthyroid after one radioiodine dose had significantly higher pretreatment serum T4 concentrations, had significantly larger volumes of hyperfunctioning thyroid tissue on scintigrams, and were more likely to have received oral radioiodine therapy. Because of these results, the authors concluded that administering a dose of radioiodine based solely on the volume of hyperfunctioning thyroid tissue estimated from a pertechnetate scan may be inadequate for those patients with extremely elevated serum T4 concentrations or large thyroid glands. The authors also concluded that oral radioiodine administration should not be recommended for feline hyperthyroidism.
Novel treatment options
Two alternative treatment methods are ethanol and heat ablation of thyroid nodules. These methods will probably have limited use in treating hyperthyroidism given the success of medical and radioiodine therapy.
Ethanol ablation
Ethanol ablation of thyroid nodules has been tried as a novel nonmedical treatment for hyperthyroidism in cats. This procedure is done under ultrasound guidance with the animal heavily sedated. In one case report, an 8-year-old female spayed domestic shorthaired cat was treated with intrathyroid injections of ethanol.10 The cat had been only partially responsive to 131I treatment four weeks before. The percutaneous ethanol injections were given four times over six weeks. The cat became acutely dyspneic shortly after the last treatment. Bilateral laryngeal paralysis was diagnosed and surgically corrected. Repeated measurements of serum T4 concentrations and thyroid scintigraphy showed a marked decrease in the size and function of the treated thyroid lobe.
A more recent paper described the use of ethanol ablation in four cats.11 The cats had increased serum T4 concentrations, a palpable thyroid nodule, and clinical signs of hyperthyroidism. Unilateral disease was identified with nuclear scintigraphy, and an enlarged single thyroid mass was found in each cat by using ultrasonography. The thyroid mass volumes were 0.20, 0.33, 0.74, and 0.84 cm3. The cats received intravenous propofol to prevent movement during the 10-minute injection procedure. Ultrasound guidance was used to place a 27-ga needle into the thyroid mass. Ethanol (96%) was slowly injected until it diffused throughout the mass or an injection volume of half the calculated mass volume was given. All four cats received a single injection, and within 48 hours serum T4 and free T4 concentrations became normal or subnormal. These hormone concentrations remained below or within the reference range during the six-month study. The owners reported that their cats' clinical signs of hyperthyroidism resolved within one week of the treatment. The cats did not exhibit clinical signs of hypothyroidism or require thyroid supplementation. Nuclear scintigraphy done three months after the injection procedure revealed normal results in one cat and faint residual increased pertechnetate uptake in three cats. Severe serum chemistry profile abnormalities or clinical complications were not seen after the ethanol injection or during the study. The owners noticed a transient voice change in two of the cats within a few days of the injection, but it resolved six to eight weeks later.
Heat ablation
A recent study evaluated ultrasound-guided heat ablation of thyroid tissue in nine cats with hyperthyroidism.12 While treatment was successful in lowering total T4 concentrations in all cats, the mean duration of euthyroidism was only four months, and hyperthyroidism recurred in all cats within 18 months after treatment.
HYPERTHYROIDISM THERAPY AND RENAL DISEASE
Many cats successfully treated for hyperthyroidism experience a decrease in renal function, though only a small percentage experience severe azotemia or clinical signs. The first study to evaluate the effects of treating hyperthyroidism on renal function involved 58 cats.13 Urine specific gravity and serum creatinine, blood urine nitrogen (BUN), and T4 concentrations were measured before and 30 and 90 days after the cats' hyperthyroidism was treated with radioactive iodine, methimazole, or bilateral thyroidectomy. Thirty and 90 days after treatment, the mean serum creatinine and BUN concentrations were significantly higher than pretreatment concentrations. The mean serum creatinine, BUN, and T4 concentrations did not differ among groups before treatment or 30 and 90 days after treatment. This finding was important as it showed that the treatment itself was not the problem; instead, the worsening azotemia may have resulted from reversal of the hyperthyroid and hypermetabolic state. Reducing serum T4 concentrations by treating hyperthyroidism may cause azotemia in older cats with chronic renal disease. The authors concluded that it may be prudent to treat azotemic (or, in fact, all) hyperthyroid cats with methimazole until you can determine whether correcting the hyperthyroid state will cause a clinically relevant reduction in renal function.
Similar results were found in another study of 22 cats treated with radioiodine alone.14 Serum T4, serum creatinine, and BUN concentrations and urine specific gravity were measured before treatment and six and 30 days after treatment. The glomerular filtration rate (GFR) was measured by using nuclear medicine imaging techniques for all 22 cats before treatment and six days after treatment for 21 of the cats. Significant decreases in serum T4 concentrations occurred six days after treatment, but the changes in GFR and serum creatinine and BUN concentrations were not significant. Thirty days after treatment, significant increases in BUN and serum creatinine concentrations occurred as well as further significant decreases in serum T4 concentrations. Nine cats were in renal failure before treatment, and 13 cats were in renal failure 30 days after treatment. These 13 cats included eight of the nine cats in renal failure before treatment (one cat was no longer in renal failure after treatment) and five cats not previously in renal failure. (Renal failure was defined as a BUN concentration greater than 30 mg/dl or a serum creatinine concentration greater than 1.8 mg/dl with a concurrent urine specific gravity of less than 1.035.) Evaluations after 30 days for nine of these 13 cats indicated that all remained in renal failure. The authors analyzed the cats' pretreatment GFR measurements as a predictor of posttreatment renal failure and derived a value of 2.25 ml/kg/min as a point of maximum sensitivity (100%) and specificity (78%). Fifteen of 22 cats had pretreatment GFR measurements below 2.25 ml/kg/min. These 15 cats included all nine cats in renal failure and five cats with normal renal clinicopathologic test results before treatment. Thirty days after treatment, 13 of these 15 cats were in renal failure. The two cats that were not in renal failure had persistently increased serum T4 concentrations. Seven of the 22 cats had pretreatment GFR measurements greater than 2.25 ml/kg/min, and none of these seven cats was in renal failure 30 days after treatment. The authors concluded that significantly decreased renal function occurs after treating hyperthyroidism, and this decrease is clinically important in cats with renal disease. Measuring GFR before treating hyperthyroidism is valuable in detecting subclinical renal disease and in predicting which cats may have clinically important reductions in renal function.
In another study, researchers examined the effects of methimazole therapy on renal function in cats with naturally occurring hyperthyroidism.15 Twelve hyperthyroid cats and 10 clinically normal (control) cats were studied. Renal function was assessed with a single-injection plasma iohexol clearance test (a measurement of GFR), along with routine serum chemistry profiles and urinalyses. After the initial evaluation, all hyperthyroid cats were treated with methimazole at a starting dose of 5 mg given orally every 12 hours. Dose adjustments were made until euthyroidism was achieved. The mean pretreatment GFR, as estimated by the plasma iohexol clearance test, was significantly higher for the hyperthyroid cats than for the control cats. Control of hyperthyroidism significantly decreased the GFR when compared with pretreatment values. No significant difference was noted between the mean GFR for the posttreatment hyperthyroid cats and the mean GFR for the control cats. In the hyperthyroid group, the mean increases in BUN and serum creatinine concentrations and the mean decrease in urine specific gravity after treatment were not statistically significant when compared with pretreatment values. Two of the 12 hyperthyroid cats developed abnormally high serum creatinine concentrations after treatment. Both of these cats exhibited isosthenuria on pretreatment urinalyses and had posttreatment GFR values of less than 1 ml/kg/min. The authors thought that posttreatment reductions in GFR most likely unmasked latent renal dysfunction in these two cats. The authors concluded that when treating hyperthyroid cats suspected to have renal dysfunction, it is prudent to conduct a trial course of meth imazole with follow-up serum chemistry profiles and urinalyses before selecting a nonreversible therapy (e.g. thyroidectomy, radioactive iodine).
The effects of hyperthyroidism on renal function were also evaluated in a group of 10 normal adult cats in which hyperthyroidism was induced with exogenous administration of T4.16 Baseline serum T4 measurements, complete blood counts, serum chemistry profiles, urinalyses, and nuclear medicine assessments of GFR and effective renal plasma and renal blood flow were performed. The cats were then given T4 (50 B5g/kg subcutaneously) daily for 30 days to induce hyperthyroidism. The clinicopathologic tests and nuclear medicine studies were repeated 30 days later, and the results revealed significant increases in T4 concentrations, GFR, and effective renal blood flow and significant decreases in serum creatinine and BUN concentrations.
The clinical importance of these studies seems to be that hyperthyroidism induces an artificial state of increased GFR, resulting in a decrease in serum BUN and creatinine concentrations. Treating hyperthyroidism (whether with surgery, methimazole, or radioiodine) reduces the GFR and causes an unmasking or progression of underlying chronic renal disease. Except for measuring GFR before treatment, no reliable clinical sign or laboratory test helps practitioners predict which cat might exhibit a clinically important deterioration in renal function after therapy. It is important to emphasize that the number of cats with severe or clinically relevant declines in renal function posttreatment is small. However, based on these studies, it is prudent to initiate low-dose methimazole therapy (or other forms of medical therapy) with renal and thyroid function monitoring after seven to 10 days before performing surgery or radioiodine therapy.
SUMMARY
The method chosen to treat a hyperthyroid cat depends on several factors, including cost, convenience, and the patient's current health. Since hyper th y roidism can mask other illnesses such as renal disease, practitioners should conduct follow-up evaluations with physical examinations and laboratory testing to monitor thyroid hormone concentrations and kidney function over time. Cardiovascular parameters should also be examined periodically, especially if hypertension or heart enlargement were noted at the time of diagnosis. The frequency of checkups will depend on the treatment method chosen and the patient's response to therapy.
David S. Bruyette, DVM, DACVIM
VCA West Los Angeles Animal Hospital
1818 S. Sepulveda Blvd.
West Los Angeles, CA 90025
REFERENCES
1. Flanders, J.A.: Surgical options for the treatment of hyperthyroidism in the cat. J. Feline Med. Surg. 1 (3):127-134; 1999.
2. Padgett, S.L. et al.: Efficacy of parathyroid gland autotransplantation in maintaining serum calcium concentrations after bilateral thyroparathyroidectomy in cats. JAAHA 34 (3):219-224; 1998.
3. Trepanier, L.A. et al.: Efficacy and safety of once versus twice daily administration of methimazole in cats with hyperthyroidism. JAVMA 222 (7):954-958; 2003.
4. Bucknell, D.G.: Feline hyperthyroidism: Spectrum of clinical presentations and response to carbimazole therapy. Aust. Vet. J. 78 (7):462-465; 2000.
5. Murray, L.A.; Peterson, M.E.: Ipodate treatment of hyperthyroidism in cats. JAVMA 211 (1):63-67; 1997.
6. Foster, D.J.; Thoday, K.L.: Use of propranolol and potassium iodate in the presurgical management of hyperthyroid cats. J. Small Anim. Pract. 40 (7):307-315; 1999.
7. Peterson, M.E.; Becker, D.V.: Radioiodine treatment of 524 cats with hyperthyroidism. JAVMA 207 (11):1422-1428; 1995.
8. Guptill, L. et al.: Response to high-dose radioactive iodine administration in cats with thyroid carcinoma that had previously undergone surgery. JAVMA 207 (8):1055-1058; 1995.
9. Forrest, L.J. et al.: Feline hyperthyroidism: Efficacy of treatment with volumetric analysis for radioiodine dose calculation. Vet. Radiol. 37:141-145; 1996.
10. Walker, M.C.; Schaer, M.: Percutaneous ethanol treatment of hyperthyroidism in a cat. Feline Pract. 26:10-12; 1998.
11. Goldstein, R.E. et al.: Ultrasound guided percutaneous ethanol injection (PEI) for the treatment of 4 cats with unilateral hyperthyroidism. Proc. ACVIM, ACVIM, Chicago, Ill., 1999.
12. Mallery, K.F. et al.: Percutaneous ultrasound-guided radiofrequency heat ablation for treatment of hyperthyroidism in cats. JAVMA 223 (11):1602-1607; 2003.
13. DiBartola, S.P. et al.: Effect of treatment of hyperthyroidism on renal function in cats. JAVMA 208 (6):875-878; 1996.
14. Adams, W.H. et al.: Changes in renal function in cats following treatment of hyperthyroidism using 131I. Vet. Radiol. Ultrasound 38 (3):231-238; 1997.
15. Becker, T.J. et al.: Effects of methimazole on renal function in cats with hyperthyroidism. JAAHA 36 (3):215-223; 2000.
16. Adams, W.H. et al.: Investigation of the effects of hyperthyroidism on renal function in the cat. Can. J. Vet. Res. 61 (1):53-36; 1997.














