Ortho or neuro? A guide to deciphering gait abnormalities
Differentiating orthopedic from neurologic conditions can be tricky, even for veterinary specialists. Heres a quick guide to reaching an accurate diagnosis based in part on gait evaluation.



monkey/stock.adobe.com
We've all had that difficult patient: You know something is wrong, but you can't tell if the problem is orthopedic or neurologic in origin. It's actually a common dilemma. Distinguishing neurologic from orthopedic gait abnormalities can give even the most seasoned practitioner trouble.
Cases that are particularly tricky to decipher involve patients that have concurrent disease (e.g. orthopedic/neurologic/systemic, polytrauma cases), chronic disease, mild or subtle findings, non–weight-bearing lameness, bilaterally symmetric orthopedic disease or unilateral/asymmetric neurologic disease.
Why are these cases so confusing?
Cases that present with concurrent disease may be confounding because clinical signs are superimposed in these patients. It isn't simply a matter of identifying which element is present or absent. Rather, you must determine the relative contributions of the various problems by first ascertaining the predominant contributor to the clinical signs. Typically the component of the problem that is most impactful on quality of life or most accessible is tackled first, and then the residual array of signs is reevaluated.
Similarly, it can be difficult to assess polytraumatized animals that are in shock and/or pain. Orthopedic and neurologic signs can be either masked or enhanced by shock, pain and/or mechanical dysfunction from traumatic injuries. Conversely, a patient may appear weak or unable to walk due to anemia or systemic disease in the absence of orthopedic or neurologic disease.
Chronic diseases may inhibit the ability to use temporal history to separate old from new clinical signs (e.g. differentiating chronic arthritis from chronic type II disk disease or slowly progressive degenerative myelopathy, distinguishing disuse and neurogenic atrophy). Diffuse disease may make it difficult to differentiate involvement of a specific system.
Mild or subtle findings can be overlooked easily on physical exam, even by an experienced specialist. Subtle findings may have a crucial influence when differentiating between a T3-L3 or C1-5 lesion (e.g. in a mildly affected wobbler syndrome case) or between orthopedic and neurologic disease (e.g. a patient with a mild or subtle neurologic deficit may be presumed normal).
Non–weight-bearing lameness presents an especially difficult dilemma when differentiating orthopedic from neurologic diseases, as the ability to obtain clues during gait evaluation is limited.
Cases that go against stereotypes are also difficult. Bilaterally symmetric orthopedic disease may be mistaken for neurologic disease because orthopedic disease is often asymmetric/focal, and neurologic disease is often symmetric. Conversely, the most common neurologic diseases encountered result from spinal cord lesions and tend to be bilateral and symmetric. Asymmetric neurologic presentations are often mistaken for orthopedic disease, especially given that lateralized neurologic signs often result from nerve root involvement, which may be associated with non–weight-bearing or partially weight-bearing lameness.
So what's a vet to do?
Perform a complete and attentive orthopedic and neurologic examination for every patient. Avoid tunnel vision and pattern spotting, and keep an open mind about the differential diagnosis. Where necessary, perform serial examinations to look for repeatable findings or trends. Attempt to decouple orthopedic from neurologic problems selectively through use of the clinical history, local joint blocks and other methods.
But aren't there more specific ways to differentiate these problems, you ask? Yes! One of the main things I like to look for is rhythmicity in the gait. To understand why this is so important, let's start from the beginning. Forget about whether it looks like a “lameness” or “neurologic.” I start by looking at the patient and asking myself whether the gait seems normal or abnormal. Firstly, this is a nice confidence booster (pats self on back for getting one right and turns to client: “Ma'am, your pet is abnormal”). Yes, I know you need more than “abnormal” to get you very far in terms of kudos, but normal versus abnormal is the first step. From there, it isn't too much more difficult (Figure 1).

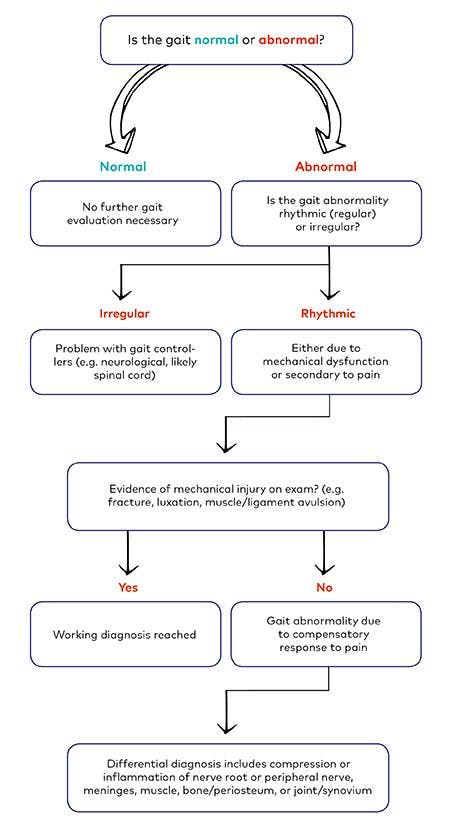
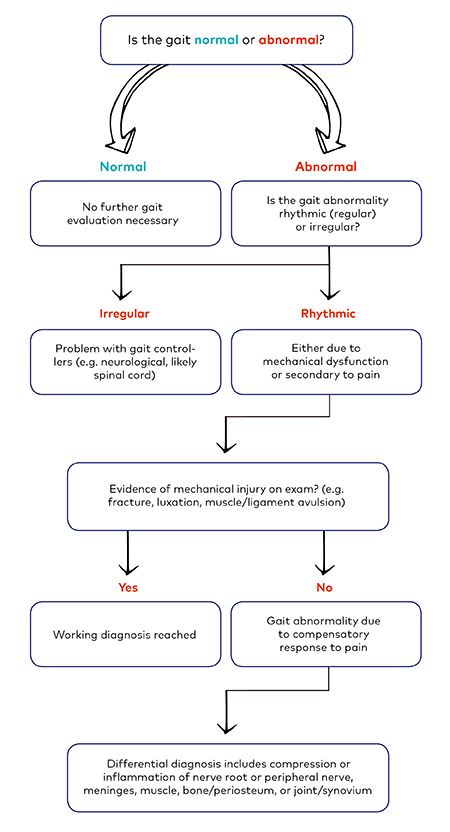
Figure 1.
There really are only three functional reasons for an abnormal gait (not etiologies, we'll get to those later):
Gait controllers are the neurologic signaling pathways that send information about movement from the brain to the effector muscles. Gait controllers are always neurologic.
Lack of mechanical support is generally musculoskeletal, such as a fracture that impairs the scaffold for support of the body, muscle avulsion, etc. These problems are fairly notable on examination, particularly in combination with gait evaluation.
Having a gait abnormality that is compensatory to pain is simply the result of something (orthopedic or neurologic) that is causing the patient pain, and as a result the gait is altered.
Don't worry about assigning a neurologic versus orthopedic etiology yet. Just try to differentiate between a problem with gait controllers versus a mechanical issue versus compensation from pain (Table 1).
Table 1. Differential diagnosis: functional causes of an abnormal gait
Gait Controllers (neurologic)
Mechanical Dysfunction (orthopedic)
Compensatory to Pain (orthopedic or neurologic)
Spinal cord disease
Brain disease
Lumbosacral disease
Junctionopathy
Polyneuropathy
Polymyopathy
Ischemic neuropathy Fracture
Ligament avulsion
Muscle avulsion
Coxofemoral luxation
Elbox luxations
Patellar luxation
Achilles tendon rupture
Neurologic
Peripheral nerve sheath tumor
Neuritis
Nerve root compression
Meningitis
Myositis
Orthopedic
Polyarthropathy
Septic arthritis
Cranial cruciate ligament disease
Osteoarthritis
Hip dysplasia
Tibial crest avulsion
Biceps tenosynovitis
Osteochondritis dissecans
Elbow dysplasia
Infraspinatus contracture
Gracilis contracture
Panosteitis
Hypertrophic osteodystrophy
So how do we do that exactly? It's easier than it seems. Look for rhythmicity in the gait:
If your patient has an abnormal gait, is the abnormality rhythmic? With every step, can you snap your fingers or clap your hands and predict exactly the rhythm with which the patient will take its next abnormal step (Video 1). Is it predictable and regular? If so, the issue is a rhythmic abnormality.
Sometimes bilaterally rhythmic gaits are difficult to discern (e.g. a dog with bilateral cruciate rupture), but the foot placement on each limb should be fairly consistent with regard to timing and to location relative to the body (e.g. alignment) (Video 2).
Rhythmic abnormalites are either mechanical or compensatory to pain. If you cannot predict the rhythm (i.e. an irregularly irregular rhythm) and it varies with every step such that you cannot predict accurately the timing or location of the next step (each step varies in terms of being base wide or base narrow, long strided or short strided (Video 3), then the problem is with the gait controllers.
As noted above, gait controllers indicate a neurologic problem (usually, but not always, related to the spinal cord). Mechanical failures are musculoskeletal by default, but a gait abnormality due to compensation from pain can be either orthopedic or neurologic. That said, the options within neurologic categories are limited. Pain (at least within the neuromusculoskeletal realm) is limited to either compression or inflammation, and only about five primary structures in those systems can be compressed or inflamed. So, a rhythmic gait abnormality is likely due to either compression or inflammation of the following structures:
- Nerve root or peripheral nerve (intervertebral disk disease, neuritis, nerve sheath tumor, etc)
- Meninges (meningitis, etc)
- Bone/periosteum (osteomyelitis, panosteitis, etc)
- Muscle (myositis, compartment injury, etc)
- Joint/synovium (osteoarthrtitis, polyarthritis, etc).
So, once you can identify which limb or limbs are abnormal, and whether the gait abnormality is rhythmic, then you've narrowed it down to fairly regional areas for further investigation. Combine this detailed clinical assessment with your exam findings, and you should have a fairly accurate differential list and a plan for diagnostic testing.
Suggested reading:
1. Dewey CW. Performing the neurologic examination. In Dewey CE (Ed.): A Practical Guide to Canine and Feline Neurology. Ames, IA: Wiley-Blackwell; 2008:53-74.
2. Gordon-Evans WJ, Evans RB, Knap KE, et al. Characterization of spatiotemporal gait characteristics in clinically normal dogs and dogs with spinal cord disease. Am J Vet Res 2009:70(12):1444-1449.
3. McDonnell JJ, Platt SR, Clayton LA. Neurologic conditions causing lameness in companion animals. Vet Clin North Am Small Anim Pract 2001;31(1):17-38.
4. Packer RA. The Small Animal Neurologic Examination: A Manual for Veterinary Students and Practitioners. Self-published; 2014. Available at: https://itunes.apple.com/us/author/rebecca-a-packer-ms-dvm-dacvim-neurology/id552636735?mt=13
5. Renberg WC. Evaluation of the lame patient. Vet Clin North Am Small Anim Pract 2001;31(1):1-16.
6. Thomas WB. Initial assessment of patients with neurologic dysfunction. Vet Clin North Am Small Anim Pract 2000;30(1):1-24.
Dr. Packer is an associate professor of neurology/neurosurgery at Colorado State University College of Veterinary Medicine and Biomedical Sciences in Fort Collins. She is active in clinical and didactic training of veterinary students and residents and has developed a comparative neuro-oncology research program at Colorado State University.














