Primary hepatic and biliary tract tumors in dogs and cats: An overview
Metastatic, disseminated, and locally infiltrative cancers, including metastatic carcinoma, melanoma, lymphoma, hemangiosarcoma, and histiocytic sarcoma, can often affect the hepatic parenchyma.
Metastatic, disseminated, and locally infiltrative cancers, including metastatic carcinoma, melanoma, lymphoma, hemangiosarcoma, and histiocytic sarcoma, can often affect the hepatic parenchyma.1,2 Compared with metastatic or secondary cancerous processes involving the liver, primary hepatobiliary tumors are uncommon in companion animals, representing only about 2.6% of canine tumors and about 5.5% of feline tumors.1,3-9 Of these, epithelial tumors of hepatic, biliary, and neuroendocrine origin as well as primary sarcomas are the most commonly diagnosed (Table 1). Other rarely documented primary hepatobiliary tumors include hepatoblastoma, plasmacytoma, and osteosarcoma in dogs and sarcomas, plasmacytoma, and myelolipoma in cats.2,4,8,10-15



Table 1 Types of Hepatobiliary Neoplasia
This article focuses on diagnosing and treating hepatobiliary epithelial tumors and primary sarcomas in dogs and cats. Because of the nonspecific clinical signs of these tumors, dogs and cats may have advanced disease at the time of diagnosis. However, given the infrequency of primary hepatobiliary tumors in both dogs and cats, differential diagnoses to consider upon identifying a hepatobiliary mass include focal hepatic nodular regeneration, a hepatic cyst (parasitic or other), a hepatic abscess (Figure 1), granuloma, hematoma, and a biliary pseudocyst.
CANINE HEPATOBILIARY TUMORS
Primary hepatobiliary tumors most commonly affect older dogs (average age = 10 to 11.1 years).1,16,17 In general, no sex or breed predisposition has been identified.1 In dogs with primary hepatobiliary tumors, hematologic and biochemical changes tend to be variable and nonspecific; however, some biochemical abnormalities may increase the index of suspicion for specific tumor types (e.g. marked hyperlipasemia is supportive of a diagnosis of pancreatic or hepatic neoplasia) or may hint at overall disease extent.18 Serum alpha-fetoprotein may help you differentiate between neoplastic and nonneoplastic hepatic disorders, and higher concentrations of serum alpha-fetoprotein may differentiate hepatocellular carcinomas from cholangiocarcinomas.19,20 Compared with metastatic hepatic tumors, primary hepatic tumors are more likely to cause hypoglycemia, hypoproteinemia, and elevations in alkaline phosphatase (ALP) and alanine transaminase (ALT) activities and are less likely to cause hyperbilirubinemia.16



Figure 1. The liver from a 5-year-old mixed-breed dog that had an acute onset of lethargy, vomiting, and elevated liver enzyme activities. A large, yet confined area of necrosis affects one liver lobe, with gross morphologic abnormalities consistent with a focal hepatic abscess.
Perform a thorough clinical evaluation, including a complete blood count, serum chemistry profile, and urinalysis, in all dogs suspected of having neoplastic hepatobiliary disease. The results of additional diagnostic tests such as coagulation profiles, hepatic function tests (bile acids, ammonia concentrations), diagnostic imaging (ultrasonography, computed tomography [CT], or magnetic resonance imaging [MRI]), cytology, and tissue biopsy may be crucial in guiding therapeutic decisions (see text titled "Definitively diagnosing hepatobiliary tumors in dogs and cats" at the end of the article).
Although most canine hepatobiliary tumors are histologically malignant, surgical excision remains the recommended treatment if anatomically feasible.1 Up to 75% of a normal liver can be resected without impairing hepatic function, and complete parenchymal regeneration can be achieved within eight weeks after surgical resection.21 For dogs with hepatobiliary tumors treated with surgery alone, the prognosis can be influenced by the histologic type, the degree of hepatic dysfunction, and evidence of locoregional or distant metastasis. However, for massive hepatocellular carcinoma, residual disease does not appear to negatively affect postoperative survival times.22
Despite anecdotal reports of responses to mitoxantrone and gemcitabine in veterinary medicine, systemic chemotherapy is considered relatively ineffective for treating hepatobiliary tumors.23-25 The preliminary results of chemoembolization in veterinary medicine for improved therapeutic delivery are encouraging.26 In studies in people, overexpression of the MDR1 gene (multidrug resistance gene) and its product P-glycoprotein has been demonstrated in hepatocellular carcinoma and is associated with chemoresistance.27,28 Because P-glycoprotein is normally expressed in hepatocytes as a drug efflux pump, the limited efficacy of systemic chemotherapy may be a result of altered detoxification functions of hepatocytes and biliary epithelium, allowing hepatobiliary-derived tumor cells to resist the cytotoxic effects of antineoplastic agents.
Canine hepatocellular carcinoma
Canine hepatocellular carcinoma accounts for more than 50% of all primary hepatobiliary tumors (Table 2).29 The average age of affected dogs is 11 or 12 years, with more than 80% of dogs being 10 years or older.4,21,29 Although most studies have not found a breed predisposition, 16% of the affected dogs in one report were schnauzers.4,21,29



Table 2 Characteristics of Selected Hepatobiliary Tumors
Diagnosis
Abdominal palpation may reveal hepatomegaly or a hepatic mass in about 50% of patients (Table 3).21,22 Clinical signs include weight loss, polyuria, polydipsia, vomiting, anorexia, lethargy, and, less commonly, ascites, seizures, diarrhea, and abdominal pain.21,22,29 Seizures are usually attributed to hepatic encephalopathy or hypoglycemia and, less likely, to brain metastasis.29,30

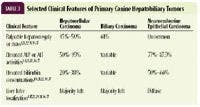
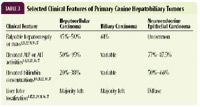
Table 3 Selected Clinical Features of Primary Canine Hepatobiliary Tumors
Although many dogs with hepatocellular carcinoma present for evaluation of obvious clinical signs of illness, nearly one-third of dogs are asymptomatic, with the discovery of hepatocellular carcinoma being an incidental finding.21,22 Nonspecific hematologic abnormalities are common and may include mild to moderate anemia and leukocytosis.21,22,29 Most affected dogs have elevations in liver enzyme activities, including ALT, aspartate aminotransferase (AST), and ALP; however, hyperbilirubinemia is present in only 20% to 38% of patients.1,21,22,29 Hypoglycemia can be associated with hepatocellular carcinoma; however, documentation of a low blood glucose concentration is relatively rare (less than 5%) in dogs without any overt clinical signs.22 Despite the low frequency of hypoglycemia in asymptomatic dogs, hepatocellular carcinoma should remain a top differential diagnosis in dogs with known hepatic neoplasia and clinical signs of hypoglycemia.30 Furthermore, in dogs with extensive or advanced hepatocellular carcinoma, hepatic function may be markedly compromised, resulting in prolonged coagulation times in up to 21% of patients.21,22 To minimize the likelihood of excessive and life-threatening hemorrhage in these patients, consider the possibility of altered hemostasis before biopsy or surgical intervention. In patients at risk for excessive hemorrhage, consider fine-needle aspiration and cytology as a less invasive option than liver biopsy for obtaining a definitive diagnosis of hepatocellular carcinoma.
Hepatobiliary tumors in people
Classification
Most canine hepatocellular carcinomas arise from the left side of the liver, particularly the left lateral lobe.4,17,22,29 Traditionally, hepatocellular carcinoma in dogs may be classified as one of three forms: massive, nodular, or diffuse. More than 50% of hepatocellular carcinomas are massive, usually presenting as a solitary mass involving one liver lobe.29 The reported frequency of adjacent liver lobe involvement in dogs with massive hepatocellular carcinoma is variable. Although previous reports demonstrated additional liver lobe involvement in 20% to 80% of dogs at necropsy, more recent work involving 42 dogs undergoing surgical excision for massive hepatocellular carcinoma found no evidence of additional masses in any patient.1,22,29 Similarly, previous postmortem studies reported a 22% to 36% distant metastatic rate (lymph nodes, peritoneum, lungs), while more recent studies report less than 5% metastasis at diagnosis.1,22,29 The discrepancy between the presence of metastases at diagnosis vs. at necropsy would suggest that early detection and surgical intervention may result in a longer local disease-free interval and may reduce the risk of metastatic dissemination.
The nodular form of hepatocellular carcinoma is characterized by nodules in multiple liver lobes and accounts for 16% to 29% of canine hepatocellular carcinoma cases, while the diffuse form accounts for only 10% of cases. Early reports demonstrated an extremely high metastatic rate (93% to 100%) for these forms of canine hepatocellular carcinoma.1,29 However, the reported metastatic rate, surgical inoperability, and suspected overall poor prognosis are based on necropsy findings, and earlier clinical detection may result in a better outcome.
Treatment
While there is an apparent lack of good treatment options for nodular or diffuse hepatocellular carcinoma, massive hepatocellular carcinoma can often be treated effectively with excisional surgery. However, because of the anatomical location and proximity to large blood vessels, the intraoperative mortality rate approaches 5% in dogs surgically treated for massive hepatocellular carcinoma.22 Overall, survival times for dogs treated surgically are generally favorable, with many patients achieving long survival times. In one study, more than 50% of dogs surgically treated for massive hepatocellular carcinoma were alive one year after surgery (range = one day to greater than 1,025 days).21 In another study, dogs treated with surgical excision had a longer median survival time (> 1,460 days, mean 409 days) than those treated with conservative medical management only (median survival time 270 days, mean 162 days) had.22
Although surgery is considered the best treatment for massive hepatocellular carcinoma, postoperative survival times may be dictated by primary tumor location since patients with neoplasms resected from the left, central, or right liver lobes appear to have differing median survival times—1,460+, 795+, or 365 days, respectively.22 The difference in median survival times is likely due to variables including the difficulty of the surgical approach and the tumor's proximity to vasculature.
Canine biliary carcinoma
Biliary carcinomas include biliary cystadenocarcinomas and, rarely, carcinomas of the gallbladder. These tumors account for 21.8% of primary hepatobiliary tumors (Table 2).31 The average age of affected dogs is 10 to 11.4 years; almost two-thirds of the dogs are more than 10 years old.4,17,32 Females are overrepresented in multiple studies, and one report suggested an increased risk for biliary tumors in Labrador retrievers, as well as spayed dogs compared with intact females.33
More than half of the affected dogs have palpable hepatomegaly or a mass (Table 3), and icterus is apparent in up to 23% of the affected dogs.1,31 The clinical signs are comparable to those seen with other hepatobiliary tumors, although vomiting may be less common.4 Trends in biochemical findings conflict among studies; however, elevations in ALT and ALP activities and bilirubin concentrations may be seen.1,4
The malignant transformation of biliary epithelium more commonly occurs within the hepatic parenchyma, and it has been reported that the development of intrahepatic tumors is three times as likely as the development of extrahepatic tumors.33 Necropsies have shown that biliary carcinomas tend to possess an aggressive phenotype, capable of spreading to adjacent liver lobes, regional lymph nodes, and distant sites in dogs.1,33,34 While the pathogenesis for biliary carcinoma in dogs remains poorly defined, chronic inflammation may be involved, as suggested by the association of carcinoma development and concurrent parasitic infestations.33,34
Similar to hepatocellular carcinomas, biliary carcinomas tend to affect the left lateral liver lobe in most patients, and about 50% of biliary carcinomas are solitary lesions (massive form).1,4,17,31 When anatomically feasible, these tumors are typically treated with surgical excision. Negative prognostic factors established in a recent evaluation of dogs undergoing surgery for extrahepatic biliary tract neoplasia included septic bile peritonitis, an elevated creatinine concentration, and an elevated partial thromboplastin time.35
Canine neuroendocrine epithelial tumors
Tumors arising from the neuroendocrine epithelium (carcinoids) account for 13% of primary canine hepatobiliary tumors (Table 2) and have been demonstrated to most frequently involve hepatic parenchyma and to sporadically involve biliary tissue. No breed or sex predilection has been established; however, these neoplasms typically affect younger dogs (average 8 to 9.8 years)—more than two-thirds of the dogs are less than 10 years old.4,36,37 About 20% of dogs exhibit icterus, and in contrast to other tumor histologic types, hepatomegaly is often not detected on physical examination.36,37 The clinical signs mimic those of other hepatobiliary tumors; however, ascites are more common.4
Hematologic changes may include anemia and leukocytosis. Trends in liver enzyme activities are more consistent for neuroendocrine carcinomas than they are for biliary carcinomas—more than 75% of the affected dogs have elevated ALT and ALP activities, and nearly two-thirds are hyperbilirubinemic (Table 3). Unlike hepatocellular carcinomas and biliary carcinomas, carcinoid tumors are most often diffuse in nature and affect most of the liver parenchyma.4,36,37 At necropsy, nearly all patients have metastasis, most commonly to the lymph nodes, peritoneum, and lungs.4,36 Despite the reported metastatic nature and suspected poor prognosis of carcinoid tumors based on necropsy studies alone, early detection may allow better treatment options, such as resection, and, thus, the true prognosis remains undetermined.
Canine hepatic sarcomas
Sarcomas account for less than 15% of primary hepatobiliary tumors in dogs (Table 2).4 In general, primary hepatic sarcomas occur in older dogs (average 11 years), and females are at an increased risk. The clinical signs are comparable to those of other hepatobiliary diseases, with variable changes in hematologic and biochemical parameters (Table 3).4
Although various primary sarcomas (leiomyosarcoma, fibrosarcoma, myxosarcoma, liposarcoma) have been reported, the most common sarcomas to affect the hepatic parenchyma are hemangiosarcoma (Figure 2) and histiocytic sarcoma.2,4 Therapy for these two sarcomas may depend on determining whether the tumor arises primarily from the liver or whether it is metastatic, which may be suggested by the size of the hepatic lesion. Surgical excision of a primary hepatic hemangiosarcoma or excisional biopsy of suspected hepatic metastases from a primary splenic hemangiosarcoma may be considered and should be followed by systemic chemotherapy with a doxorubicin-based protocol.

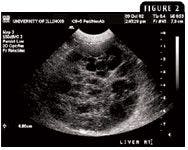
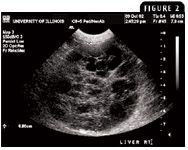
Figure 2. An ultrasonogram of a 9-year-old male castrated German shepherd presenting for evaluation of episodic weakness and lethargy. A large liver mass is identified, characterized by a mixed echogenic pattern with multiple hypoechoic cavitated lesions. Microscopic examination confirmed the liver tumor to be hemangiosarcoma.
FELINE HEPATOBILIARY TUMORS
Although neoplastic processes have been documented in cats as young as 2 years old, hepatobiliary tumors are primarily a disease of older cats (average 12 years). Hepatobiliary tumors may be classified as either malignant or benign, with malignant tumors more commonly arising in younger cats (average 9 years) compared with benign tumors (average 14.5 years) (Table 2).38 In contrast to dogs in which most hepatobiliary tumors are malignant, up to 65% of primary hepatobiliary tumors in cats are benign (Figure 3).38-40 More than 50% of feline hepatobiliary tumors are incidental findings at surgery or necropsy.38
Figure 3. The exploratory laparotomy findings from a 7-year-old female spayed domestic shorthaired cat presented for evaluation of subtle weight loss, elevated liver enzyme activities, and icterus. The results of the histologic examination of the resected hepatic mass were consistent with a benign hepatic adenoma.
Clinical signs, if demonstrated by affected cats, are variable and may include anorexia, weight loss, lethargy, intermittent vomiting, and icterus.39-41 Although complete staging is typically recommended to confirm metastatic disease in cats, interpret additional hepatic lesions with caution, as 16% to 25% of cats with hepatobiliary tumors may have multiple benign lesions throughout the liver (see text titled "Definitively diagnosing hepatobiliary tumors in dogs and cats" at the end of the article).39,40
Feline biliary adenocarcinomas
The average age of cats with biliary adenocarcinomas and cystadenocarcinomas (Figures 4A & 4B) is 13.3 to 14.5 years, and male cats are overrepresented (Table 2).41-43 Despite a palpable abdominal mass or hepatomegaly in about half of affected cats, elevations in liver enzyme activities and bilirubin concentrations are uncommon (Table 4).38,40-42 Although many cats may present for clinical signs attributable to the hepatobiliary system, 38% of cats are asymptomatic.42
Figure 4A. An ultrasonogram of a 12-year-old male castrated domestic shorthaired cat presented for evaluation of reduced appetite and weight loss of six months duration. A mixed echogenic liver mass is identified, possessing multiple cystlike cavities.
Definitive treatment recommendations for cats with biliary adenocarcinoma or cystadenocarcinomas remain to be determined, but consider surgical resection if anatomically feasible. In two case series, surgical excision resulted in minimal complications, and no local recurrence was observed in the 12 to 44 months of postsurgical follow-up.43,44 Based on these limited studies, surgical excision may provide prolonged disease-free intervals and high quality-of-life scores in cats with biliary adenocarcinomas and carcinomas of the biliary tract.



Figure 4B. The postmortem findings from the same cat reveal a multilobulated mass involving the liver parenchyma and arising from the biliary epithelium. The results of the histologic examination of the hepatic lesion were consistent with a biliary cystadenocarcinoma.
Feline neuroendocrine epithelial tumors
Feline tumors arising from the neuroendocrine epithelium of hepatic and biliary tissues have been reported.45 The average age is 9 years, and males are overrepresented (Table 2). The clinical signs are similar to those seen with other hepatobiliary diseases; however, less than 30% of cats have a palpable abdominal mass (Table 4). More than 50% of cats with biliary neuroendocrine tumors are icteric, with elevations in AST, ALP, and ALT activities. Conversely, cats with hepatic neuroendocrine tumors rarely have marked biochemical changes.



Table 4 Selected Clinical Features of Primary Feline Hepatobiliary Tumors*
Treatment for feline neuroendocrine tumors remains anecdotal, but attempted surgical resection has been reported. In one study, more than 80% of cats died or were euthanized soon after surgery. Metastasis—most often involving the lymph nodes, lungs, or intestines or with evidence of peritoneal carcinomatosis—was identified in all the cats in which necropsy information was available.45
Feline hepatocellular carcinomas
Feline hepatocellular carcinomas account for up to 17% of hepatobiliary tumors. Clinical findings, diagnostic tests, and treatment are similar to that of other hepatobiliary tumors. Pulmonary and splenic metastases have been rarely documented.38,39
Feline hepatic sarcomas
Primary hepatic sarcomas are uncommon in cats, but fibrosarcoma, hemangiosarcoma, osteosarcoma, leiomyosarcoma, and rhabdomyosarcoma have been reported.8,14,15,38
CONCLUSION
Although specific clinical signs such as a palpable liver mass or icterus may indicate a primary hepatobiliary tumor, signs and abnormalities in blood work may often be nonspecific. Thus, dogs and cats with hepatobiliary neoplasia may have advanced disease at the time of diagnosis. Cytology, tissue biopsy, and the use of advanced imaging such as MRI and CT can help you determine whether liver lesions are benign or malignant. In dogs, most tumors are malignant, while benign tumors are more common in cats.
Although a patient's prognosis depends on many factors, including tumor histologic type, the degree of parenchymal involvement, and metastatic disease, excisional surgery and supportive care remain the primary therapeutic options for all hepatobiliary tumors in dogs and cats. Through the use of advanced imaging modalities, hepatobiliary tumors may be more readily diagnosed in companion animals. In turn, the early detection of liver cancer may permit prompt institution of treatment, ultimately improving the survival outcomes for dogs and cats with liver cancer.
Jackie Wypij, DVM
Timothy M. Fan, DVM, DACVIM (oncology, internal medicine)
Louis-Philippe de Lorimier, DVM, DACVIM (oncology)
Department of Veterinary Clinical Medicine
College of Veterinary Medicine
University of Illinois
Urbana, IL 61802
REFERENCES
1. Trigo FJ, Thompson H, Breeze RG, et al. The pathology of liver tumours in the dog. J Comp Pathol 1982;92:21-39.
2. Hammer AS, Sikkema DA. Hepatic neoplasia in the dog and cat. Vet Clin North Am Small Anim Pract 1995;25:419-435.
3. MacVean DW, Monlux AW, Anderson PS Jr, et al. Frequency of canine and feline tumors in a defined population. Vet Pathol 1978;15:700-715.
4. Patnaik AK, Hurvitz AI, Lieberman PH. Canine hepatic neoplasms: a clinicopathologic study. Vet Pathol 1980;17:553-564.
5. Dorn CR, Taylor DO, Frye FL, et al. Survey of animal neoplasms in Alameda and Contra Costa Counties, California. I. Methodology and description of cases. J Natl Cancer Inst 1968;40:295-305.
6. Whitehead JE. Neoplasia in the cat. Vet Med Small Anim Clin 1967;62:357-358.
7. Schmidt RE, Langham RF. A survey of feline neoplasms. J Am Vet Med Assoc 1967;151:1325-1328.
8. Patnaik AK, Liu SK, Hurvitz AI, et al. Nonhematopoietic neoplasms in cats. J Natl Cancer Inst 1975;54:855-860.
9. Engle GC, Brodey RS. A retrospective study of 395 feline neoplasms. J Am Anim Hosp Assoc 1969;5:21-31.
10. Shiga A, Shirota K, Shida T, et al. Hepatoblastoma in a dog. J Vet Med Sci. 1997;59:1167-1170.
11. Aoki M, Kim T, Shimada T, et al. A primary hepatic plasma cell tumor in a dog. J Vet Med Sci 2004;66:445-447.
12. Langenbach A, Anderson MA, Dambach DM, et al. Extraskeletal osteosarcomas in dogs: a retrospective study of 169 cases (1986-1996). J Am Anim Hosp Assoc 1998;34:113-120.
13. Larsen AE, Carpenter JL. Hepatic plasmacytoma and biclonal gammopathy in a cat. J Am Vet Med Assoc 1994;205:708-710.
14. Minkus G, Hillemanns M. Botryoid-type embryonal rhabdomyosarcoma of liver in a young cat. Vet Pathol 1997;34:618-621.
15. Dhaliwal RS, Johnson TO, Kitchell BE. Primary extraskeletal hepatic osteosarcoma in a cat. J Am Vet Med Assoc 2003;222:340-342, 316.
16. Strombeck DR. Clinicopathologic features of primary and metastatic neoplastic disease of the liver in dogs. J Am Vet Med Assoc 1978;173:267-269.
17. Evans SM. The radiographic appearance of primary liver neoplasia in dogs. Vet Radiol 1987;28:192-196.
18. Quigley KA, Jackson ML, Haines DM. Hyperlipasemia in 6 dogs with pancreatic or hepatic neoplasia: evidence for tumor lipase production. Vet Clin Pathol 2001;30:114-120.
19. Lowseth LA, Gillett NA, Chang IY, et al. Detection of serum alpha-fetoprotein in dogs with hepatic tumors. J Am Vet Med Assoc 1991;199:735-741.
20. Yamada T, Fujita M, Kitao S, et al. Serum alpha-fetoprotein values in dogs with various hepatic diseases. J Vet Med Sci 1999;61:657-659.
21. Kosovsky JE, Manfra-Marretta S, Matthiesen DT, et al. Results of partial hepatectomy in 18 dogs with hepatocellular carcinoma. J Am Anim Hosp Assoc 1989;25:203-206.
22. Liptak JM, Dernell WS, Monnet E, et al. Massive hepatocellular carcinoma in dogs: 48 cases (1992-2002). J Am Vet Med Assoc 2004;225:1225-1230.
23. Ogilvie GK, Obradovich JE, Elmslie RE, et al. Efficacy of mitoxantrone against various neoplasms in the dog. J Am Vet Med Assoc 1991;198:1618-1621.
24. Moore AS, Kitchell BE. New chemotherapy agents in veterinary medicine. Vet Clin North Am Small Anim Pract 2003;33:629-649, viii. Review.
25. Shimada M, Takenaka K, Kawahara N, et al. Chemosensitivity in primary liver cancers: evaluation of the correlation between chemosensitivity and clinicopathological factors. Hepatogastroenterology 1996;43:1159-1164.
26. Weisse C, Clifford CA, Holt D, et al. Percutaneous arterial embolization and chemoembolization for treatment of benign and malignant tumors in three dogs and a goat. J Am Vet Med Assoc 2002;221:1430-1436, 1419.
27. Huang CC, Wu MC, Xu GW, et al. Overexpression of the MDR1 gene and P-glycoprotein in human hepatocellular carcinoma. J Natl Cancer Inst 1992;84:262-264.
28. Park JG, Lee SK, Hong IG, et al. MDR1 gene expression: its effect on drug resistance to doxorubicin in human hepatocellular carcinoma cell lines. J Natl Cancer Inst 1994;86:700-705.
29. Patnaik AK, Hurvitz AI, Lieberman PH, et al. Canine hepatocellular carcinoma. Vet Pathol 1981;18:427-438.
30. Leifer CE, Peterson ME, Matus RE, et al. Hypoglycemia associated with nonislet cell tumor in 13 dogs. J Am Vet Med Assoc 1985;186:53-55.
31. Patnaik AK, Hurvitz AI, Lieberman PH, et al. Canine bile duct carcinoma. Vet Pathol 1981;18:439-444.
32. Strafuss AC. Bile duct carcinoma in dogs. J Am Vet Med Assoc 1976;169:429.
33. Hayes HM Jr, Morin MM, Rubenstein DA. Canine biliary carcinoma: epidemiological comparisons with man. J Comp Pathol 1983;93:99-107.
34. Chang HP. Hepatic clonorchiasis and carcinoma of the bile duct in a dog. J Pathol Bacteriol 1965;89:365-367.
35. Mehler SJ, Mayhew PD, Drobatz KJ, et al. Variables associated with outcome in dogs undergoing extrahepatic biliary surgery: 60 cases (1988-2002). Vet Surg 2004;33:644-649.
36. Patnaik AK, Lieberman PH, Hurvitz AI, et al. Canine hepatic carcinoids. Vet Pathol 1981;18:445-453.
37. Patnaik AK, Newman SJ, Scase T, et al. Canine hepatic neuroendocrine carcinoma: an immunohistochemical and electron microscopic study. Vet Pathol 2005;42:140-146.
38. Lawrence HJ, Erb HN, Harvey HJ. Nonlymphomatous hepatobiliary masses in cats: 41 cases (1972 to 1991). Vet Surg 1994;23:365-368.
39. Patnaik AK. A morphologic and immunocytochemical study of hepatic neoplasms in cats. Vet Pathol 1992;29:405-415.
40. Post G, Patnaik AK. Nonhematopoietic hepatic neoplasms in cats: 21 cases (1983-1988). J Am Vet Med Assoc 1992;201:1080-1082.
41. Nyland TG, Koblik PD, Tellyer SE. Ultrasonographic evaluation of biliary cystadenomas in cats. Vet Radiol Ultrasound 1999;40:300-306.
42. Adler R, Wilson DW. Biliary cystadenoma of cats. Vet Pathol 1995;32:415-418.
43. Trout NJ. Surgical treatment of hepatobiliary cystadenomas in cats. Semin Vet Med Surg (Small Anim) 1997;12:51-53.
44. Trout NJ, Berg RJ, McMillan MC, et al. Surgical treatment of hepatobiliary cystadenomas in cats: five cases (1988-1993). J Am Vet Med Assoc 1995;206:505-507.
45. Patnaik AK, Lieberman PH, Erlandson RA, et al. Hepatobiliary neuroendocrine carcinoma in cats: a clinicopathologic, immunohistochemical, and ultrastructural study of 17 cases. Vet Pathol 2005;42:331-337.
Definitively diagnosing hepatobiliary tumors in dogs and cats
In addition to performing complete blood counts, serum chemistry profiles, urinalyses, coagulation profiles, and hepatic function tests when investigating possible hepatobiliary tumors in dogs and cats, you will need to perform diagnostic imaging. Cytology and histology are needed to make a definitive diagnosis.
Figure 1. A ventrodorsal abdominal radiograph of a 7-year-old dalmatian presented for evaluation of elevated liver enzyme activities and painless abdominal distention. A large cranial abdominal mass effect (white arrows) with caudal displacement of the intestines is identified. Surgical biopsy confirmed a diagnosis of massive hepatocellular carcinoma.
Imaging
Abdominal radiography and ultrasonography as well as advanced imaging modalities can be used to help identify an abdominal mass.
Radiography
In clinical practice, abdominal radiography is often the most convenient method for evaluating hepatomegaly or a palpable abdominal mass. A common radiographic pattern associated with hepatobiliary tumors is a cranial abdominal mass with caudal and lateral displacement of the stomach.1,2 Although a mass effect is infrequently detected with biliary carcinomas, most hepatomas (hepatocellular adenomas) and up to 100% of hepatocellular carcinomas in dogs are discernible as a hepatic mass on radiographs (Figure 1).1-3 With feline hepatobiliary tumors, a mass effect is identified radiographically in only 60% of cases (Figure 2).4 Other radiographic findings consistent with hepatobiliary neoplasia in dogs include intraperitoneal fluid and mineralization within the biliary system.1,5

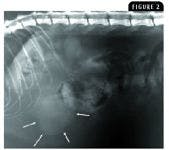
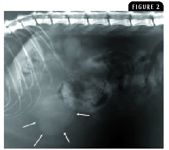
Figure 2. A lateral abdominal radiograph of a 7-year-old female spayed domestic shorthaired cat with a benign hepatic adenoma. A subtle mass effect is present (white arrows).
Ultrasonography
Abdominal ultrasonography is routinely used to identify hepatic parenchymal changes. When evaluating hepatic masses ultrasonographically, quantify and localize the masses, characterize their echogenicity, identify their distribution (solitary or diffuse), and look for evidence of cystic or vascular components. However, the ultrasonographic appearance of benign lesions such as nodular hyperplasia and many malignant lesions may be similar in dogs (Figures 3A & 3B).6-8 The difficulties in ultrasonographically differentiating between benign and malignant hepatic lesions have been recently reported. In one study, the ultrasonographic interpretation of 22 canine hepatic lesions resulted in a correct diagnosis in only 50% of cases, with more than 35% of focal benign lesions being ultrasonographically classified as neoplastic.9 Although the ultrasonographic appearances of hepatic lesions are often nonspecific, some studies have attempted to characterize ultrasonography findings most consistent with liver cancer. Some lesions identified ultrasonographically within visceral organs may take on a halo effect and are called target lesions because of a hypoechoic rim surrounding an isoechoic to hyperechoic center. Target lesions are associated with malignancy, with a positive predictive value of 74% for a focal lesion and 81% for multiple lesions.10



Figure 3A & 3B. Similar ultrasonographic appearances of a (3A) benign canine hepatocellular adenoma and (3B) malignant canine hepatocellular carcinoma (massive form). Both benign and malignant tumors produce sonographically evident mass effects, often appearing as mixed echogenic lesions.
Advanced imaging modalities
Advanced imaging modalities such as CT (Figure 4) and MRI are used in human medicine to better detect and localize hepatic lesions. MRI is an emerging modality in veterinary medicine, and a recent study in dogs demonstrated differentiation between malignant and benign hepatic lesions with a 100% sensitivity and 86% specificity. These MRI results support the notion that advanced imaging can be used to accurately differentiate between benign and malignant hepatic lesions in dogs and will perhaps, in the future, reduce unnecessary biopsy of benign liver lesions.11



Figure 4. A transverse CT image of malignant canine hepatocellular carcinoma (massive form) provides additional preoperative information about the feasibility of surgical resection. The tumor (hypointense signal) involves more than 50% of the ventral aspect of the liver.
Cytology
Cytologic examination of a sample of the hepatic mass obtained by fine-needle aspiration can provide a definitive diagnosis with minimal complications (Figure 5). However, the sensitivity of cytology for diagnosing hepatic disorders is reported to be only 33.3%, which is much lower than the sensitivity of cytology for diagnosing disease processes of other anatomical sites.12 Although hepatic cytology may have low sensitivity for accurately diagnosing nonneoplastic diseases, a good correlation exists between cytology and histology for neoplastic processes affecting the liver. The accuracy of cytology for diagnosing hepatic neoplasia is supported by two independent studies, which demonstrate 70% to 100% correlation between cytology and histology for diagnosing liver epithelial tumors.3,13
Histology
Despite the ease and relative accuracy of hepatic cytology for identifying neoplastic processes, histologic examination may be required for the definitive diagnosis of tumors that are poorly exfoliative. With ultrasound guidance, an 18-ga, spring-loaded biopsy instrument can provide adequate tissue samples for definitive diagnosis in 83.3% to 96.3% of liver samples.14-16 Perform blood work to evaluate for hemostatic disorders before doing a liver biopsy since abnormalities in platelet counts and coagulation times increase the likelihood of complications.16 A larger bore needle or a pneumatic instrument can be used to increase the chances of retrieving diagnostic samples. Liver biopsy samples may be collected with biopsy needles, ligatures, biopsy forceps, a Baker's biopsy punch, or an ultrasonically activated scalpel by using ultrasound-guided, laparoscopic, and surgical approaches. When determining the appropriate biopsy method for a patient, consider the suspected underlying disease, concurrent disease processes, anesthetic risks, and potential for complications such as infection and hemorrhage. In general, all biopsy techniques are associated with minimal hemorrhage when evaluated in normal dogs.14

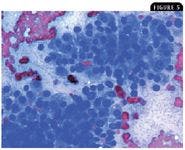

Figure 5. A photomicrograph of a fine-needle aspirate from a large solitary liver mass in a 9-year-old male castrated Labrador retriever presented for evaluation of abdominal discomfort and inappetence. The cells have a moderate rim of basophilic cytoplasm with a large round nucleus and prominent nucleoli, consistent with a well-differentiated hepatocellular carcinoma (WrightâÂÂs stain; 500X). (Photograph courtesy of Dr. Anne Barger.)
REFERENCES
1. Evans SM. The radiographic appearance of primary liver neoplasia in dogs. Vet Radiol 1987;28:192-196.
2. Kosovsky JE, Manfra-Marretta S, Matthiesen DT, et al. Results of partial hepatectomy in 18 dogs with hepatocellular carcinoma. J Am Anim Hosp Assoc 1989;25:203-206.
3. Liptak JM, Dernell WS, Monnet E, et al. Massive hepatocellular carcinoma in dogs: 48 cases (1992-2002). J Am Vet Med Assoc 2004;225:1225-1230.
4. Lawrence HJ, Erb HN, Harvey HJ. Nonlymphomatous hepatobiliary masses in cats: 41 cases (1972 to 1991). Vet Surg 1994;23:365-368.
5. Bromel C, Smeak DD, Leveille R. Porcelain gallbladder associated with primary biliary adenocarcinoma in a dog. J Am Vet Med Assoc 1998;213:1137-1139, 1131.
6. Stowater JL, Lamb CR, Schelling SH. Ultrasonographic features of canine hepatic nodular hyperplasia. Vet Radiol 1990;31:268-272.
7. Feeney DA, Johnston GR, Hardy RM. Two-dimensional, gray-scale ultrasonography for assessment of hepatic and splenic neoplasia in the dog and cat. J Am Vet Med Assoc 1984;184:68-81.
8. O'Brien RT, Iani M, Matheson J, et al. Contrast harmonic ultrasound of spontaneous liver nodules in 32 dogs. Vet Radiol Ultrasound 2004;45:547-553.
9. Vörös K, Vrabély T, Papp L, et al. Correlation of ultrasonographic and pathomorphological findings in canine hepatic diseases. J Small Anim Pract 1991;32:627-634.
10. Cuccovillo A, Lamb CR. Cellular features of sonographic target lesions of the liver and spleen in 21 dogs and a cat. Vet Radiol Ultrasound 2002;43:275-278.
11. Clifford CA, Pretorius ES, Weisse C, et al. Magnetic resonance imaging of focal splenic and hepatic lesions in the dog. J Vet Intern Med 2004;18:330-338.
12. Cohen M, Bohling MW, Wright JC, et al. Evaluation of sensitivity and specificity of cytologic examination: 269 cases (1999-2000). J Am Vet Med Assoc 2003;222:964-967.
13. Roth L. Comparison of liver cytology and biopsy diagnoses in dogs and cats: 56 cases. Vet Clin Pathol 2001;30:35-38.
14. Vasanjee SC, Bubenik LJ, Hosgood G, et al. Evaluation of hemorrhage, sample size, and collateral damage for five hepatic biopsy methods in dogs. Vet Surg 2006;35:86-93.
15. Barr F. Percutaneous biopsy of abdominal organs under ultrasound guidance. J Small Anim Pract 1995;36:105-113.
16. Bigge LA, Brown DJ, Penninck DG. Correlation between coagulation profile findings and bleeding complications after ultrasound-guided biopsies: 434 cases (1993-1996). J Am Anim Hosp Assoc 2001;37:228-233.















