Senior dental care: Never too old for good dental health
With individualized anesthesia protocols and appropriate monitoring, veterinary dental procedures are safer than ever before. Now, all senior patients can enjoy the benefits of good dental care.



Photo source: Getty ImagesThe prevalence of periodontal disease increases as age increases and as body weight decreases (large dogs versus small dogs).1 Similar to other chronic processes, particularly ones with tissue loss (gingival and bone), this disease is likely to worsen without intervention until the final phase of periodontal disease-tooth loss. The coinfluence relationship of dental disease with diabetes and renal disease underscores the importance of addressing issues in senior animals before they cause more problems.2
Dentistry and blood work can help support each other's efforts: if a recent senior diagnostic screening has been performed, now would be a good time to get the patient's dental work accomplished. If dental care is needed, now would be a good time to update the patient's laboratory values, especially if this screening had been declined in the past. While not common, it is possible to pick up on underlying, occult disease when performing a patient's preoperative screening.
As patients get long in the tooth
Periodontal disease has an increased incidence in senior animals, as do any of the dental conditions that can increase over time, such as tooth resorption or stomatitis in cats. Extensive periodontal disease that has destroyed mandibular bone at the level of the first molar can lead to pathologic fractures, sometimes bilaterally, that have insufficient osseous structure for stabilization (Figure 1).

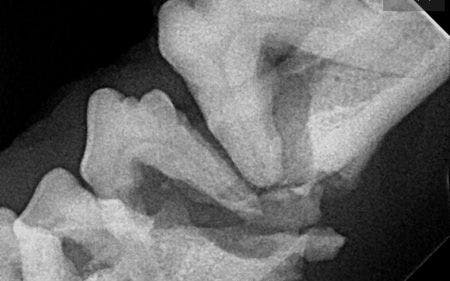
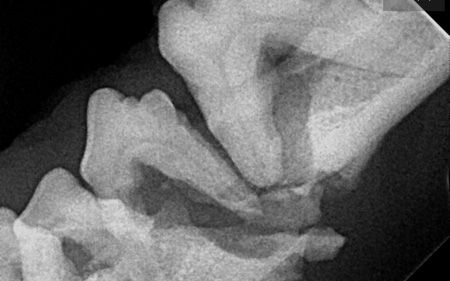
Figure 1: An intraoral radiograph showing a pathologic fracture of the left mandible due to periodontal bone loss. (Photo courtesy of Dr. Heidi Lobprise)
Senior cats may exhibit a thickening of the alveolar bone surrounding the canine teeth, especially the maxillary ones, with a concurrent super-eruption of the teeth, making them look longer than normal (Figure 2). This chronic osteitis or alveolitis may be minor, with periodontal management sufficient for treatment. If the tooth is mobile or the surrounding tissues are inflamed, extraction may be the best route.



Figure 2: Thickened alveolar bone surrounding the canine teeth, with a concurrent super-eruption of the teeth. (Photo courtesy of Dr. Heidi Lobprise)
Oral tumors are also seen more frequently in senior patients, and early detection and identification of any masses can provide the only possibility for adequate treatment. In dogs, melanocytic tumors, fibrosarcomas and squamous cell carcinomas are some of the most frequent masses found, while the three forms of squamous cell carcinoma (gingival, lingual, tonsillar) are the most common masses found in cats.
Cocurrent concerns to chew on
The increase in periodontal disease in senior animals should warrant professional care, but the presence of comorbidities can make the necessary anesthetic procedures potentially risky. In rare instances, the disease is so severe or unresponsive to management that dental care should be avoided completely.
However, most cases can be evaluated preoperatively to identify underlying issues, and those identified disease processes can be treated to return the patient to a more stable condition to decrease the risk the anesthetic procedure would entail. In each patient, the risk of retaining the dental disease and its potential effects on the rest of the body should be weighed against the risk of treatment. Typically, the benefits of treatment outweigh the risks.
The drill before you drill
Individualized treatment plans are essential for senior and geriatric patients: from the preoperative evaluation and stabilization therapy (if needed) to the immediately preoperative period and perioperative time frames. Many comparisons can be made to guidelines for people for dental procedures, including the benefit of preoperative laboratory screening, but we have to realize that our patients cannot give us details about how they are feeling.
Anesthetic risk classification
Identifying the patient's American Society of Anesthesiologists (ASA) physical status classification is a good starting point when evaluating patients in the mature, senior or geriatric categories. This classification will help you determine which assessments should be performed.
Patients classified as ASA I or II might require basic blood work, a urinalysis and an electrocardiogram (ECG), while patients classified as ASA III, IV or V might require additional diagnostic testing. Urine output (1 to 2 mg/kg/hour is normal) monitoring is seldom performed but can provide beneficial information.
Preoperative medications and fasting
It is important to discuss preoperative medications with owners, including identifying which medications could affect anesthetic and analgesic drugs. Decisions may have to be made about which medications can be given on the day of the procedure.
Fasting should be discussed with owners of diabetic patients. If a small morning meal is necessary to maintain glucose concentrations, it should be no more than half the typical amount, and induction of anesthesia should be delayed by at least four to six hours. The morning insulin dose should also be halved, though water can be offered until presented at the clinic. Blood glucose concentrations should be checked at induction and recovery; if a procedure is prolonged, intraoperative concentrations may be checked as well. A constant-rate infusion (CRI) of regular insulin and dextrose fluids can be considered to maintain a consistent hyperglycemia.3
For most patients, food should be stopped the evening before, but small amounts of water can be given until they are admitted to the hospital.
Antibiotics
Antibiotic use and selection will always generate plenty of discussion. Again, while dental recommendations for people should be considered, our patients have the additional complication of anesthesia, with possible hypovolemia, hypotension or hypothermia, so each patient's treatment plan should be individualized.
If the patient has some systemic risk (e.g. cardiac disease, borderline renal disease), it may be appropriate to give that patient a broad-spectrum antibiotic (e.g. amoxicillin-clavulanic acid) just before the procedure (four to six hours) or to administer intravenous ampicillin or amoxicillin during the procedure. In my experience, in some patients with extreme dental infection, a course of antibiotics in the weeks or days before the procedure, such as clindamycin, has greatly improved the health of the patient's dental tissues-and also the health of the patient.
Pain management
Another important aspect of dental care is pain management. Appropriate administration of preoperative agents can reduce the patient's anxiety and stress in the preoperative stage, which could have a positive effect on stress-induced immunosuppression. If a patient is given appropriate, effective preoperative, multimodal analgesia combined with local and regional blocks, then the dose of general anesthetic needed for the patient can usually be reduced significantly. If nonsteroidal anti-inflammatory drugs are given (only to patients with no evidence of renal malfunction), perfusion with fluids is important.
For local and regional anesthetic blocks, the total dose should be calculated, particularly in small dogs and cats. Bupivacaine (0.5%) premixed with epinephrine (1:200,000) provides analgesic effects for longer with some hemorrhage control but should not be given to patients with contraindications (cardiac arrhythmias, hyperthyroidism). It also needs to be placed 10 to 20 minutes before the extraction or periodontal procedure for maximum effectiveness. Lidocaine does not last as long but provides analgesic effects more quickly.
While you're at it: perioperative care
Perfusion before and throughout the procedure is critical in dental anesthetic cases to maintain adequate blood volume, particularly for renal function. An initial appropriate intravenous crystalloid fluid bolus (5 to 10 mg/kg) may be provided preoperatively with 5 to 10 mg/kg/hour for a maintenance dose. Cardiac patients might have decreased ability to compensate for normal and excessive fluid volumes, so monitor patients closely for any signs of overhydration, including increased pulmonary sounds or even abnormal packed cell volume. The intraoperative replacement of fluids will offset the loss of water from evaporation and third space losses into traumatized tissues and will even replace volume lost to hemorrhage in some cases.
Maintaining a patient's body temperature during a dental procedure can be quite challenging: many patients are old and small, and the oral cavity is constantly wet or being rinsed. Geriatric patients in particular can have exaggerated hypothermia with a decreased basic metabolism rate. Body temperatures less than 98 F (36.7 C) can alter mentation, the patient's immune competency and wound healing. Decreased body temperature can also affect recovery time.
Keep the patient as dry as possible and provide patient warming devices when appropriate. Passive and active surface rewarming with warm water blankets, air warming devices or conductive fabric blankets can be helpful, as can active core rewarming with warmed isotonic fluids.
Patient monitoring
The reason I have confidence in safe anesthesia is the combination of individualized analgesia and anesthesia protocols and the level of patient monitoring that can be provided. General anesthesia depresses many systems that may already be compromised-respiratory, cardiovascular, central nervous, thermoregulatory, hepatic and renal, to name a few. Monitoring should be constant throughout the procedure and into the postoperative period, where most unexpected deaths occur.
And keep in mind that with all the advances in monitoring equipment available, the best monitor is still a good technician. Observing the general parameters and readings from monitoring equipment provides the best assessment of the depth of anesthesia and indicates when there is a need for intervention. Heart and respiration rates recorded every five minutes can be combined with pulse oximetry and blood pressure values, carbon dioxide concentrations, capnograph readings, body temperature and continuous ECG readouts. Central nervous system evaluation of the muscle tone of the jaw and eye position or palpebral reflex are more subtle indicators of anesthetic depth.
Lengthy procedures
A dental procedure can be lengthy, which may lead to concerns about decreasing body functions as time goes on, particularly in senior patients. Maintaining perfusion and blood pressure with fluids can decrease body temperature, as can moisture associated with the dental procedure. Keep anesthetic concentrations as low as possible to help maintain blood pressure without waking the patient.
Some situations-either because of the patient's body systems, the length of time needed or the extent of treatment needed-could necessitate staging the procedure, completing a portion of the surgery at a later date.
Anticipate emergencies
Emergency situations should be anticipated ahead of time with printed protocols for the common drugs that may be needed in such events (for an emergency drug calculator, click here). Regular monitoring should highlight any trends in parameter changes that could precede an emergent event, and if patient response is inadequate, immediate recovery should be instigated.
A gentle recovery
Patient monitoring should not end when the anesthesia is turned off or when the endotracheal tube is removed. In fact, since the patient is not observed as closely as during the perioperative period, recovery is often when adverse events happen, sometimes leading to the patient's death.
Brachycephalic patients, in particular, should be closely monitored. Because the challenges to their air passages return once the tube is removed, the tube should remain in place for as long as possible.
Any swelling, hemorrhage or pain flare-up can add to the patient morbidity. In patients with emergent delirium, a very low dose of dexmedetomidine (no more than 0.1 ml in a large dog) may be administered (if it is not contraindicated) to help relieve anxiety, stress and pain for a smoother, slower recovery. If a patient shows marked pain beyond that, additional opioids may be required.
If the patient had issues with hypotension during the procedure, fluid administration and even inotropes may be considered postoperatively, with close monitoring. Bradycardia may be present because of the effects of anesthesia, as well as any prolongation of hypothermia. If any medication (e.g. an alpha2-adrenergic agonist) was given, a reversal agent is recommended, and an anticholinergic may be given with caution. Providing a safe means of keeping the patient warm and dry is also recommended.
Monitoring urine output-either a specific measurement or encouraging conscious voiding-can help you determine if additional fluids are needed. With small patients and, certainly, those with diabetes mellitus, monitoring blood glucose concentrations during and after anesthesia can point out those patients that might need additional treatment.
Follow-up care: Not just lip service
Returning the patient to normal function as quickly as possible helps the recovery process. Discuss postoperative medications from analgesics to antibiotics with owners for proper administration. Patients should be encouraged to eat and drink small amounts that evening, though the food may need to be softened. Supplemental feeding may be necessary, including anything from syringe feeding to a percutaneous endoscopic gastrostomy tube, depending on the patient. A phone recheck the next day and a physical examination in two weeks allow you to continue monitoring the patient and develop a plan for ongoing management.
A last bite of advice
While senior animals may present with particular circumstances that make anesthesia planning more complicated, in most instances, appropriate patient evaluation and care will provide an opportunity for good dental care. If dental health can be improved in a senior patient, its overall health is likely to improve as well.
References
1. Harvey CE, Shofer FS, Laster L. Association of age and body weight with periodontal disease in North American dogs. J Vet Dent 1994;11(3): 94-105.
2. Preshaw PM, Alba AL, Herrera D, et al. Periodontitis and diabetes: a two-way relationship. Diabetologia 2012; 55(1):21-31.
3. Van Nice E. Management of multiple dental infections in a dog with diabetes mellitus. J Vet Dent 2006;23(1):18-25.
Heidi Lobprise, DVM, DAVDC
Main Street Veterinary Hospital and Dental Clinic
4100 Kirkpatrick Lane
Flower Mound, TX 75028










 in general practice")




