Clinical Rounds: Recurrent mast cell tumors in a boxer
See how these veterinary specialists and residents used various therapies to produce a good outcome in this case.
OVERVIEW
Olya A. Smrkovski, DVM, DACVIM (oncology)



Dr. Olya A. Smrkovski
Mast cell tumors comprise 16% to 21% of all skin tumors and represent the most common cutaneous neoplasm in dogs (Figure 1).1 Predisposed breeds include boxers, Boston terriers, Labrador retrievers, beagles, and schnauzers.1 Metastatic rates vary but tend to be correlated with the histologic grade of the primary tumor. Low-grade cutaneous mast cell tumors have a metastatic rate of 10% to 15%, whereas high-grade cutaneous mast cell tumors have metastatic rates > 50%.1 Common sites of metastasis include regional lymph nodes, the liver, and the spleen. A mast cell tumor can be definitively diagnosed on cytologic examination of a fine-needle aspirate, while histopathologic examination of an excised tumor or biopsy sample provides tumor grade and margin assessment.
1. The gross appearance of a mast cell tumor at the base of the caudal pinna in a dog.
Case Presentation
A 6-year-old 57.6 lb (26.2 kg) spayed female boxer was presented to The University of Tennessee Veterinary Medical Center for staging and treatment of multifocal cutaneous masses on its left ear. On physical examination, three alopecic, ulcerated nodules were found on the left pinna. Two of the nodules (5 x 3 x 2.5 cm and 0.5 x 0.5 x 0.5 cm) were located at the base of the lateral aspect of the pinna, and the third nodule (5.2 x 3.2 x 2 cm) was near the tip of the ear.
Cytologic examination of fine-needle aspirates obtained from each nodule was diagnostic for mast cell tumor. No abnormalities were found on bloodwork, thoracic and abdominal radiographic examinations, or abdominal ultrasonographic examination. No evidence of metastasis was found on cytologic examination of fine-needle aspirates of the left mandibular lymph node, liver, and spleen. Thus, surgical excision of the tumors was recommended.
Initial treatment
A left pinnectomy was performed, including 3-cm margins around the two tumors at the base of the ear pinna and about one-third of the vertical ear canal. Histologic evaluation of the resected tissue indicated completely excised grade III mast cell tumors with 12 mitotic figures in 10 high-power fields.
Adjuvant chemotherapy was recommended because of the high tumor grade, and 14 days after the surgery a vinblastine and prednisone chemotherapy protocol (Table 1) was initiated.2
Table 1: Protocol for Using Vinblastine and Prednisone to Treat Mast Cell Tumors in Dogs
Second presentation
Six weeks later, while still receiving vinblastine and prednisone, the dog developed another mast cell tumor on its left lip. In addition, an enlarged left prescapular lymph node was noted on physical examination. Cytologic examination of an aspirate obtained from the lymph node was consistent with metastatic mast cell tumor. The left mandibular lymph node was not enlarged on physical examination and did not contain cytologic evidence of metastatic mast cell tumor. Chemotherapy with vinblastine and prednisone was discontinued, and chemotherapy with masitinib mesylate (Kinavet-CA1—AB Science) (12.5 mg/kg orally every 24 hours),3 diphenhydramine (2 mg/kg orally every 8 hours), and famotidine (0.5 mg/kg orally every 12 hours) was initiated.
Follow-up and further developments
At a recheck appointment one month after masitinib treatment was initiated, the dog's disease was stable. No side effects from the masitinib were noted. At the two-month recheck, the left prescapular lymph node and the mast cell tumor on the left lip remained unchanged in size; however, a new cutaneous mass (3.5 x 1.8 x 0.5 cm) was found in the left axilla. Cytologic examination of a fine-needle aspirate of this mass was diagnostic for mast cell tumor.
Additional chemotherapy. Because masitinib had not prevented tumor progression, the owners were offered treatment with either lomustine or toceranib phosphate (Palladia—Pfizer Animal Health).4,5 They elected to treat the dog with toceranib (2.75 mg/kg orally every 48 hours). The dog was concurrently treated with famotidine, maropitant citrate (Cerenia—Pfizer Animal Health), metronidazole, and sucralfate because of a reported high incidence of gastrointestinal toxicity of toceranib phosphate.5
Two weeks later, the dog became lethargic and anorectic and developed three new mast cell tumors. Additionally, the mast cell tumor on the left lip had grown in size by about 30%.
Toceranib was discontinued, and treatment with lomustine (70 mg/m2) and concurrent high-dose vitamin C (250 mg/kg orally every 24 hours) was started. It is important to point out that there is no literature supporting the use of high-dose vitamin C for the treatment of canine mast cell tumors but that therapy was initiated based on anecdotal clinical observations of response of gross mast cell tumors to this form of therapy by one of the attending clinicians.6 The lomustine proved to be ineffective since two weeks later two new mast cell tumors were found, and the tumor on the left lip had grown larger.
Masitinib reinstituted. Because of the lack of better treatment options, masitinib therapy (12.5 mg/kg orally every 24 hours) was reinstituted, since the dog had its longest interval of stable disease (about two months) while receiving this drug. Two weeks after masitinib treatment was reinstituted, the owners reported resolution of the dog's anorexia and lethargy. The high-dose vitamin C was discontinued. The dog was reevaluated four weeks after restarting on masitinib, and complete resolution of all gross mast cell tumors was noted on physical examination. Masitinib therapy was continued in an effort to prevent recurrence of mast cell tumor formation.
Seven months after masitinib treatment was reinstituted, the dog developed a mild neutropenia (1,900/μl), so the drug's frequency was decreased to every 48 hours. The dog subsequently developed a mast cell tumor on its chin, however, so the masitinib frequency was increased to every 24 hours after resolution of the neutropenia.
Case outcome. Two years later, the dog is in complete remission while remaining on masitinib therapy. The dog currently has no evidence of macroscopic mast cell tumors and is monitored every two months for neutropenia, increases in liver enzyme activities, and proteinuria, which are the reported side effects of masitinib.3
MEDICAL PERSPECTIVE
Bethany Sabatino, DVM
Dr. Bethany Sabatino
Mast cell tumors are unique among neoplasms in that they often secrete a variety of vasoactive substances (e.g. heparin, histamine, serotonin) and proteases that can lead to an increased propensity for gastrointestinal ulceration, local or systemic bleeding or bruising, local tissue damage, and hypotension.7 Many of these substances and a variety of inflammatory mediators are also produced in nonneoplastic mast cells as a protective response.8
A key to optimizing the health of all patients with mast cell tumors (especially those with large or metastatic tumors) is daily administration of antihistamines (both H1 and H2 antagonists).9 Proton-pump inhibitors such as omeprazole can be an acceptable alternative to H1 antagonists.10 Conversely, unless a coagulopathy is documented, specific therapy addressing the heparin release from mast cell tumors is typically not necessary. Although plasma therapy in patients with concurrent mast cell tumor and coagulopathy may or may not be effective, it should be considered.11 Therapy with protamine sulfate to treat a coagulopathy may also be beneficial in some dogs.1
RADIOLOGY PERSPECTIVE
Laura Hammond, DVM



Dr. Laura Hammond
In patients with mast cell tumors, the goals of diagnostic imaging are to identify the extent of metastatic disease, guide tissue sampling, and screen for comorbidities. Consistent with these goals, baseline imaging of dogs with mast cell tumors in our institution includes three-view thoracic radiography, abdominal radiography, and abdominal ultrasonography.
Although mast cell tumors do not generally cause nodular pulmonary metastases,12 thoracic radiography allows assessment of intrathoracic lymph nodes and screening for concurrent abnormalities. We use abdominal radiographs for the most accurate assessment of organomegaly.
Abdominal ultrasonography evaluates the echogenicity and architecture of the liver, spleen, and regional lymph nodes and facilitates targeted tissue sampling. As the ultrasonographic appearance of organs infiltrated with malignant mast cells may be normal, ultrasound-guided fine-needle aspiration of the liver and spleen is recommended, regardless of ultrasonographic findings, in all patients suspected of having aggressive forms of mast cell neoplasia.13
clinical pathology perspective
Carolyn Grimes, DVM
Dr. Carolyn Grimes
Cytologic samples from canine mast cell tumors are typically highly cellular and have a predominance of granulated mast cells (round to oval cells with abundant, fine to coarse, metachromatic cytoplasmic granules). Mast cells may be present individually or in aggregates and may be associated with low to moderate numbers of scattered eosinophils and plump, often pleomorphic, fusiform cells. The background of the smear often contains blood and variable numbers of scattered mast cell granules from ruptured cells.
Samples containing a highly mixed population of cells and those obtained from noncutaneous lesions (e.g. spleen, lymph node) should be interpreted cautiously, as moderate or sometimes high numbers of mast cells may be present as part of a reactive or inflammatory process. Many resources that may aid in cytologic evaluation of canine cutaneous mast cell tumors are available.14 Canine cutaneous mast cell tumors are graded based on histopathologic not cytopathologic criteria (see anatomic pathology perspective).
When mast cells are heavily granulated and present in high numbers, cytologic interpretation is not challenging. However, some mast cell tumor samples may contain cells with few or faint granules, which may reflect poor differentiation of the neoplastic cells or may be associated with staining methodology. Mast cell granules may stain poorly or not at all when an aqueous-based stain such as a modified Wright's stain (Diff Quik—Dade Behring) or most other dip stains is used.15
2. This fine-needle aspirate from a cutaneous axillary mass in a dog contains individualized round cells with low numbers of scattered eosinophils and neutrophils and a small amount of blood. The round cells are large with pale cytoplasm, which frequently contains a moderate amount of fine, faint metachromatic granulation. They demonstrate moderate anisocytosis and anisokaryosis, and occasional binucleation (inset) (Wrightâs stain [aqueous], 100X).
This case
Fine-needle aspiration of multiple skin lesions and a lymph node in the dog in this case revealed a predominance of large, pale round cells with variable amounts of very fine, faint cytoplasmic granulation (Figure 2).
Anatomic pathology perspective
Jorden Manasse, BVMS
Dr. Jorden Manasse
When submitting a potential mast cell tumor for histopathologic diagnosis, it is important to define surgical margins as medial/lateral, proximal/distal, dorsal/palmar, or cranial/caudal. This can be done by using sutures placed along a selected margin. Histologic margins are correlated with outcome: a recent study examining Grade I and II mast cell tumor histologic margins found that with lateral margins of ≥ 10 mm and deep margins of ≥ 4 mm, no tumor recurrence or metastatic disease was observed.16
Histopathologic examination
Histopathologic examination usually provides a definitive diagnosis. Mast cell tumors are generally well demarcated, nonencapsulated dermal masses containing round cells arranged in cords and sheets admixed with variable numbers of eosinophils. Extension into the subcutis is common, but extension to the dermal-epidermal junction is rare.17 Mast cell granules may be highlighted in poorly differentiated tumors by using a metachromatic toluidine blue special stain, by staining for chymase activity, or by performing immunohistochemistry for the presence of tryptase antigen.18 Of the three, a toluidine blue stain is the easiest and fastest to perform.
3. The histologic appearance of the tumor in this case showing a pleomorphic population of round cells within the dermis. The neoplastic mast cells are poorly differentiated, with multiple binucleated cells and occasional multinucleated cells present. Eosinophils are seen scattered among the neoplastic population (hematoxylin and eosin stain, 400X; bar = 50 μm).
Grading
Recently, a new two-tier grading system (low grade, high grade) was proposed over the Patnaik three-tier grading system.19 This study found that classifying mast cell tumors as low or high grade provided the best prognostic information for survival and that dogs with high-grade MCTs had a median survival time of < 4 months and dogs with low-grade MCTs had a median survival time of > 2 years.20
This case
In the case study discussed, a Grade III mast cell tumor was diagnosed, which would be considered high grade under the new grading scheme. The deep dermis contained a well-demarcated unencapsulated mass of round cells showing marked cellular pleomorphism with numerous binucleated and few multinucleated cells (Figure 3). The mitotic rate was 12/10 hpf (400X), and eosinophils were scattered throughout the mass. A toluidine blue stain showed variable positive staining of granules within the neoplastic population (Figure 4).

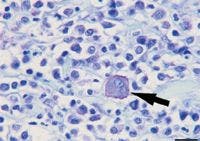
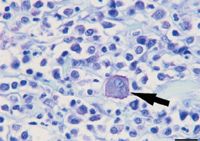
4. The histologic appearance of the tumor in this case showing cytoplasmic granules of a binucleated cell (arrow) and many surrounding neoplastic cells that stain magenta on a blue background with the toluidine blue stain (400X; bar = 50 μm).
SURGICAL PERSPECTIVE
Karen M. Tobias, DVM, MS, DACVS



Dr. Karen M. Tobias
Surgical resection is the treatment of choice for mast cell tumors amenable to wide excision. Margins required for complete resection depend on the tumor grade. Patnaik19 Grade I mast cell tumors are completely excised with margins 1 cm wide and one fascial plane deep (Table 2). Complete excision of Patnaik Grade II mast cell tumors may require margins 2 cm wide and one fascial plane deep; however, complete excision is possible with 1-cm-wide margins in up to 75% of dogs.21,22 Since tumor grade is usually unknown before surgery, clinicians will usually attempt to achieve 2-cm margins.
Table 2: Patnaik Grading System for Canine Cutaneous Mast Cell Tumors*
Remarkably, local recurrence rates after incomplete resection of Patnaik Grade II mast cell tumors is 5% to 23%,23 suggesting that mast cells found along margins of some samples are likely recruited healthy cells rather than neoplastic ones.
If the ability to attain adequate surgical margins is questionable because of peritumoral edema or ill-defined borders, use of preoperative glucocorticoids can be considered. In one study, 70% of dogs showed a reduction in tumor size when treated with prednisone for a median of 10 days before surgery.24 Mean tumor volume and maximal diameter decreased 53% and 35%, respectively, in dogs receiving low-dose prednisone (1 mg/kg [0.45 mg/lb] orally ever 24 hours) and 78% and 49%, respectively, in dogs receiving high-dose prednisone (2.2 mg/kg [1 mg/lb] orally every 24 hours). The difference in response based on dose was not significantly different.24 The effect of preoperative corticosteroid administration on tumor grade has not been determined.
MEDICAL ONCOLOGY PERSPECTIVE
Richard A. Chetney, Jr., DVM
Dr. Richard A. Chetney, Jr.
The two most common chemotherapy options we use for canine cutaneous mast cell tumors include combination oral prednisone and injectable vinblastine25 or oral lomustine.4 However, other cytotoxic chemotherapies have been shown to have efficacy against mast cell tumors (Table 3).
Table 3: Cytotoxic Chemotherapy Drugs with Documented Clinical Efficacy Against Canine Mast Cell Tumors
A recent study demonstrated that a new water-soluble (micellar) formulation of paclitaxel (1 mg/ml; Paccal Vet—Oasmia Pharmaceutical AB) was safe and had a higher confirmed overall response rate than lomustine in dogs with advanced nonresectable mast cell tumors.26 The biologic overall response rate to lomustine in this study (10%) was much lower than in previous reports, but the endpoint for assessment of response to the micellar paclitaxel was 14 weeks vs. six weeks for the lomustine.4,26
Tyrosine kinase inhibitors
Oral small molecule tyrosine kinase inhibitors toceranib phosphate and masitinib mesylate are two novel FDA-approved drugs for treating canine mast cell tumors. They competitively inhibit the ATP-binding site of the various members of the split-kinase receptor family, preventing receptor phosphorylation and downstream cell signaling.27 Toceranib targets primarily Kit, VEGF, and PDGFR.5,27 Masitinib's targets include Kit, PDGFR, and EGFR.3
In a study of 145 dogs with recurrent and nonresectable cutaneous mast cell tumors, the overall response rate to toceranib was 43% (21 dogs had a complete response, 41 had a partial response).5 In a double-blind, randomized, placebo-controlled phase III clinical trial of dogs with gross mast cell tumor disease, masitinib significantly increased time to tumor progression compared with placebo, especially when masitinib was used as the initial therapy.3
Prognostic factors
Prognostic indicators for mast cell tumors include histologic grade, mitotic index, tumor characteristics such as growth rate and ulceration, the tumor's location, the patient's breed, the clinical stage of disease, tumor-related clinical signs, and tumor recurrence after surgical excision.1,28 The presence of c-kit gene mutation, Kit protein localization status, and cellular proliferation indices (Ki67, AgNOR, PCNA) also carry prognostic significance.23,29
The Kit receptor tyrosine kinase plays an important role in mast cell tumor pathogenesis. Several studies have shown that 20% to 30% of canine mast cell tumors carry a Kit mutation, which results in constitutive activation of this receptor.30,31 Kit mutations were found more frequently in higher Patnaik grade mast cell tumors and were associated with increased risk of local tumor recurrence and metastasis.29,32
This case
The status of Kit mutation was unknown in the dog in this case. The fact that the disease originally progressed in face of masitinib followed by complete response to the drug is difficult to explain and would be interesting to investigate. A recent report demonstrated that combinations of two tyrosine kinase inhibitors can produce synergistic inhibition of growth and proliferation of canine C2 mastocytoma cell line in vitro.33 Tyrosine kinases inhibitors have also been reported to produce synergism in people with myeloid malignancies.33 It is unknown what effect the exposure to toceranib before reinstitution of masitinib therapy had on this dog's mast cell tumors.
RADIATION ONCOLOGY PERSPECTIVE
Nathan Lee, DVM, DACVR (radiation oncology)
Dr. Nathan Lee
It has been well-established that adjuvant radiation therapy can be used for local control of incompletely excised grade II mast cell tumors.34,35 A study of 32 dogs with incompletely excised grade II mast cell tumors reported an 88% disease-free survival at two to five years after treatment with definitive radiation therapy with a total dose of 54 Gy over 39 days.34 Another report of 37 dogs treated for incompletely excised grade II mast cell tumors showed a disease-free survival of 93% at three years for dogs treated with megavoltage or orthovoltage radiation at doses of 46.2 to 48 Gy, using several different fraction sizes and schedules.35,36
Definitive radiation therapy
Grade II mast cell tumors that have metastasized to regional lymph nodes can also benefit from definitive radiation therapy. In one report, 19 dogs with various grade tumors (16 were grade II) and regional lymph node metastasis that were treated with a radiation dose of 48 to 57 Gy to the primary tumor and the regional lymph node had a median disease-free survival time of 1,240 days.37
Prophylactic radiation therapy
If the regional lymph node is not involved, based on cytology of the draining lymph nodes, there is some controversy whether prophylactic irradiation of the regional lymph node is warranted. In a recent report, 45 dogs with stage 0 incompletely excised grade II mast cell tumors underwent definitive radiation therapy, with 24 of these patients receiving prophylactic radiation to the primary draining node. When comparisons were made between the dogs that received prophylactic irradiation of the regional lymph node and dogs that did not, no statistically significant differences were observed in disease-free survival rate, time to local recurrence, or overall survival rate.37
Combination therapy
Large mast cell tumors that cannot undergo cytoreduction by surgery can be treated with hypofractionated radiation therapy and either prednisolone alone38 or prednisone and toceranib.39 In a study from 2004, dogs treated with hypofractionated radiation therapy and prednisolone alone had an overall response rate of 88.5% and a median progression-free interval of 1,031 days.38 A newly published study looking at hypofractionated radiation therapy, prednisone, and toceranib for dogs with measurable mast cell tumors had an overall response rate of 76.4% and a median progression-free interval of 316 days.39 Unfortunately, no studies have investigated hypofractionated radiation therapy alone for gross mast cell tumors.
The current radiation protocol at The University of Tennessee for incompletely excised grade II mast cell tumors is 48 Gy given in 3 Gy fractions (Monday through Friday). We prophylactically treat the draining lymph node in dogs with stage 0 disease. If stage II disease is present, we extend the prophylactic treatment to the next lymph node in the chain (e.g. if the popliteal lymph node is involved, the internal and external iliac lymph nodes and bed are treated prophylactically).
REFERENCES
1. Thamm DH, Vail DM. Mast cell tumors. In: Withrow SJ, Vail DM, eds. Withrow & MacEwen's small animal clinical oncology. 4th ed. St. Louis, Mo: Saunders Elsevier, 2007;402–424.
2. Thamm DH, Mauldin EA, Vail DM. Prednisone and vinblastine chemotherapy for canine mast cell tumors—41 cases (1992-1997). J Vet Intern Med 1999;13(5):491-497.
3. Hahn KA, Ogilvie G, Rusk T, et al. Masitinib is safe and effective for the treatment of canine mast cell tumors. J Vet Intern Med 2008;22(6):1301-1309.
4. Rassnick KM, Moore AS, Williams LE, et al. Treatment of canine mast cell tumors with CCNU (lomustine). J Vet Intern Med 1999;13(6):601-605.
5. London CA, Malpas PB, Wood-Follis SL, et al. Multi-center, placebo-controlled, double-blind, randomized study of oral toceranib phosphate (SU11654), a receptor tyrosine kinase inhibitor, for the treatment of dogs with recurrent (either local or distant) mast cell tumor following surgical excision. Clin Cancer Res 2009;15(11):3856-3865.
6. Legendre A. The University of Tennessee College of Veterinary Medicine, Knoxville, Tenn. Personal communications, June 2012.
7. Theoharides TC, Conti P. Mast cells: the Jekyll and Hyde of tumor growth. Trends Immunol 2004;25(5):235-241.
8. Bonagura JD, Twedt DC. Mast cell tumors. In: Kirk's current veterinary therapy XIV. Philadelphia, Pa: W.B. Saunders, 2009.
9. Fox LE, Rosenthal RC, Twedt DC, et al. Plasma histamine and gastrin concentrations in 17 dogs with mast cell tumors. J Vet Intern Med 1990;4(5):242-246.
10. Pettigrew HD, Teuber SS, Kong JS, et al. Contemporary challenges in mastocytosis. Clin Rev Allergy Immunol 2010;38(2-3):125-34.
11. Howard EB, Sawa TR, Nielsen SW, et al. Mastocytoma and gastroduodenal ulceration. Gastric and duodenal ulcers in dogs with mastocytoma. Pathol Vet 1969;6(2):146-158.
12. Hume CT, Kiupel M, Rigatti L, et al. Outcomes of dogs with grade 3 mast cell tumors: 43 cases (1997-2007). J Am Anim Hosp Assoc 2011;47(1):37-44.
13. Book AP, Fidel J, Wills T, et al. Correlation of ultrasound findings, liver and spleen cytology, and prognosis in the clinical staging of high metastatic risk canine mast cell tumors. Vet Radiol Ultrasound 2011;52(5):548-554.
14. DeNicola D. Round cells. In: Cowell RL, Tyler RD, Meinkoth JH, et al., eds. Diagnostic cytology and hematology of the dog and cat. 3rd ed. St. Louis, Mo: Mosby Elsevier 2008;68-77.
15. Allison RW, Velguth KE. Appearance of granulated cells in blood films stained by automated aqueous versus methanolic Romanowsky methods. Vet Clin Pathol 2010;39(1):99-104.
16. Schultheiss PC, Gardiner DW, Rao S, et al. Association of histologic tumor characteristics and size of surgical margins with clinical outcome after surgical removal of cutaneous mast cell tumors in dogs. J Am Vet Med Assoc 2011;238(11):1464-1469.
17. Gross TL, Ihrke PJ, Walder EJ, et al. Mast cell tumors. Skin diseases of the dog and cat. 2nd ed. Oxford: Blackwell Science Ltd, 2005;853-861.
18. Fernandez NJ, West KH, Jackson ML, et al. Immunohistochemical and histochemical stains for differentiating canine cutaneous round cell tumors. Vet Pathol 2005;42(4):437-445.
19. Patnaik AK, Ehler WJ, MacEwen EG. Canine cutaneous mast cell tumor: morphologic grading and survival time in 83 dogs. Vet Pathol 1984;21(5):469-474.
20. Kiupel M, Webster JD, Bailey KL, et al. Proposal of a 2-tier histologic grading system for canine cutaneous mast cell tumors to more accurately predict biological behavior. Vet Pathol 2001;48(1):147-155.
21. Fulcher RP, Ludwig LL, Bergman PJ, et al. Evaluation of a two-centimeter lateral surgical margin for excision of grade I and grade II cutaneous mast cell tumors in dogs. J Am Vet Med Assoc 2006;228(2):210-215.
22. Simpson AM, Ludwig LL, Newman SJ, et al. Evaluations of surgical margins required for complete excision of cutaneous mast cell tumors in dogs. J Am Vet Med Assoc 2004;224(2):236-240.
23. Séguin B, Besancon MF, McCallan JL, et al. Recurrence rate, clinical outcome, and cellular proliferation indices as prognostic indicators after incomplete surgical excision of cutaneous grade II mast cell tumors: 28 dogs (1994-2002). J Vet Intern Med 2006;20(4):933-940.
24. Stanclift RM, Gilson SD. Evaluation of neoadjuvant prednisone administration and surgical excision in treatment of cutaneous mast cell tumors in dogs. J Am Vet Med Assoc 2008;232(1):53-62.
25. Thamm DH, Turek MM, Vail DM. Outcome and prognostic factors following adjuvant prednisone/vinblastine chemotherapy for high-risk canine mast cell tumour: 61 cases. J Vet Med Sci 2006;68(6):581-587.
26. Vail DM, von Euler H, Rusk AW, et al. A randomized trial investigating the efficacy and safety of water soluble micellar paclitaxel (Paccal Vet) for treatment of nonresectable grade 2 or 3 mast cell tumors in dogs. J Vet Intern Med 2012;26(3):598-607.
27. London CA. Tyrosine kinase inhibitors in veterinary medicine. Top Companion Anim Med 2009;24(3):106-112.
28. Mullins MN, Dernell WS, Withrow SJ, et al. Evaluation of prognostic factors associated with outcome in dogs with multiple cutaneous mast cell tumors treated with surgery with and without adjuvant treatment: 54 cases (1998-2004). J Am Vet Med Assoc 2006;228(1):91-95.
29. Webster JD, Yuzbasiyan-Gurkan V, Thamm DH, et al. Evaluation of prognostic markers for canine mast cell tumors treated with vinblastine and prednisone. BMC Vet Res 2008;4:32.
30. London CA, Galli SJ, Yuuki T, et al. Spontaneous canine mast cell tumors express tandem duplications in the proto-oncogene c-kit. Exp Hematol 1999;27(4):689–697.
31. Downing S, Chien MB, Kass PH, et al. Prevalence and importance of internal tandem duplications in exons 11 and 12 of c-kit in mast cell tumors of dogs. Am J Vet Res 2002;63(12):1718–1723.
32. Webster JD, Yuzbasiyan-Gurkan V, Miller RA, et al. Cellular proliferation in canine cutaneous mast cell tumors: associations with c-KIT and its role in prognostication. Vet Pathol 2007;44(3):298–308.
33. Gleixner KV, Rebuzzi L, Mayerhofer M, et al. Synergistic antiproliferative effects of KIT tyrosine kinase inhibitors on neoplastic canine mast cells. Exp Hematol 2007;35(10):1510-1521.
34. al-Sarraf R, Mauldin GN, Patnaik AK, et al. A prospective study of radiation therapy for the treatment of grade 2 mast cell tumors in 32 dogs. J Vet Intern Med 1996;10(6):376-378.
35. Frimberger AE, Moore AS, LaRue SM, et al. Radiotherapy of incompletely resected, moderately differentiated mast cell tumors in the dog: 37 cases (1989-1993). J Am Anim Hosp Assoc 1997;33(4):320-324.
36. Poirier VJ, Adams WM, Forrest, LJ, et al. Radiation therapy for incompletely excised grade II canine mast cell tumors. J Am Anim Hosp Assoc 2006;42(6):430-434.
37. Chaffin K, Thrall DE. Results of radiation therapy in 19 dogs with cutaneous mast cell tumor and regional lymph node metastasis. Vet Radiol Ultrasound 2002;43(4):392-395.
38. Dobson J, Cohen S, Gould S. Treatment of canine mast cell tumours with prednisolone and radiotherapy. Vet Comp Oncol 2004;2(3):132-141.
39. Carlsten KS, London CA, Haney S, et al. Multicenter prospective trial of hypofractionated radiation treatment, toceranib, and prednisone for measurable canine mast cell tumors. J Vet Intern Med 2012;26(1):135-141.
40. Elmslie R. Combination chemotherapy with and without surgery for dogs with high-grade mast cell tumors with regional lymph node metastases. Vet Cancer Soc Newsl 1997;20:6-7.
41. Gerritsen RJ, Teske E, Kraus JS, et al. Multiagent chemotherapy for mast cell tumours in the dog. Vet Q 1998;20:28-31.
42. Rassnick KM, Bailey DB, Russell DS, et al. A phase II study to evaluate the toxicity and efficacy of alternating CCNU and high-dose vinblastine and prednisone (CVP) for treatment of dogs with high-grade, metastatic or nonresectable mast cell tumours. Vet Comp Oncol 2010;8(2):138-152.
43. Taylor F, Gear R, Hoather T, et al. Chlorambucil and prednisolone chemotherapy for dogs with inoperable mast cell tumours: 21 cases. J Small Anim Pract 2009;50(6):284-289.
44. Rassnick KM, Al-Sarraf R, Bailey DB, et al. Phase II open-label study of single-agent hydroxyurea for treatment of mast cell tumours in dogs. Vet Comp Oncol 2010;8(2):103-111.
45. McCaw DL, Miller MA, Ogilvie GK, et al. Response of canine mast cell tumors to treatment with oral prednisone. J Vet Intern Med 1994;8(6):406-408.
46. Rassnick KM, Bailey DB, Flory AB, et al. Efficacy of vinblastine for treatment of canine mast cell tumors. J Vet Intern Med 2008;22(6):1390-1396.
47. Grant IA, Rodriguez CO, Kent MS, et al. A phase II clinical trial of vinorelbine in dogs with cutaneous mast cell tumors. J Vet Intern Med 2008;22(2):388-393.
48. McCaw DL, Miller MA, Bergman PJ, et al. Vincristine therapy for mast cell tumors in dogs. J Vet Intern Med 1997;11(6):375-378.















