Antimicrobial resistance: are we there yet? (Proceedings)
The ability of organisms to develop resistance to an antimicrobial varies with the species and strain. Many organisms remain predictably susceptible to selected drugs (eg, Brucella, Chlamydia); whereas others are becoming problematic (Pasteurella multocida).
The ability of organisms to develop resistance to an antimicrobial varies with the species and strain. Many organisms remain predictably susceptible to selected drugs (eg, Brucella, Chlamydia); whereas others are becoming problematic (Pasteurella multocida). Others have proven be a therapeutic challenge because of resistance that rapidly impairs efficacy of even new antimicrobials (E coli, Klebsiella pneumoniae, Salmonella, Staphyloccoccus aureus, Streptococcus pneumonia). In general, these organisms have developed multidrug resistance (MDR). Emergence of extended spectrum extended spectrum beta-lactamases (ESBL) is an example of the relentless adaptive nature of microbes toward designer drugs intended to preclude the advent of resistance. The ESBLs are encoded by large plasmids that can confer the information between strains as well as different species of organisms. The gene mutation confers resistance to newer cephalosporins includeing cefotaxime, ceftazidime and ceftriaxone, as well as cefpodoxime, or 4th generation including cefepime (no longer marketed in the USA); cefipime has been cited as possibly being effective against ESBL.The impact on clavulanic acid and sulbactam is not clear, although their use in place of cephalosporins appears to reduce the emergence of ESBL and may reduce the emergence of other resistant pathogens such as Clostridium difficile and vancomycin-resistant enterococci.. The ESBL are most commonly found in Klebsiella spp, E. coli or Proteus mirabilis (3.1-9.5%), but they also have been detected in other members of the Enterobacteriaceae and in Pseudomonas aeruginosa. Nosocomial organisms are another example of a source of resistant microbes. They are opportunists, probably most commonly from the environment, that cause infections as a result of medical treatment, usually in a hospital or clinic setting. Nosocomial infections are formally defined as infections arising after 48 hr of hospital admission. Because bacterial colonization by nosocomial isolates hospital occurs in the upper respiratory tract, gastrointestinal tract, urogenital tract, and skin of many patients within a few days of hospitalization, nosocomial infections not surprisingly most commonly occur in the respiratory or urinary tract or skin. Infection frequently is associated with invasive procedures. Isolates causing nosocomial infections generally are In some human intensive care units, selected isolates are characterized by resistance prevalence of 86%; resistance results in increased morbidity, mortality, and increased costs. Because nosocomial organisms are characterized by complex resistant patterns, their effective therapy often requires more expensive and potentially toxic drugs and selection clearly should be based on C&S . Nosocomial infections in veterinary critical care patients has been reviewed. The organisms associated with noscomial infections in dogs and cats have been many and diverse, varying with the report. Included (but not exclusively) are Serratia spp, Staphylococcus spp, Streptococcus spp, Klebsiella spp, Enterococcus spp, and E. coli. As in humans, predisposing factors have included catheters and previous antimicrobial therapy.
Methicillin resistance (MRSA; S. aureus; MRSP; S. intermedius [pseudintermedius] 38
Multidrug resistance is now considered the normal response to antibiotics for Gram positive cocci pneumococci, enterococcis and staphylococci. Methicillin resistance (MRSA; S. aureus; MRSP; S. intermedius [pseudintermedius]38 is indicated by the presence of the mecA gene, which encodes a mutation in PBP2a, thus reducing its affinity for the beta-lactam ring, rendering the organism resistant to all beta-lactams. The mecA gene is carried on the staphylococcal chromosomal cassette (SCC); currently 5 SCCmec have been described.39 Protectors such as clavulanic acid are ineffective.21 Detection of MRSA or MRSP on C&S generally is based on resistance to oxacillin, which is more stable than methicillin in disks used for testing. However, variability in testing methods can profoundly alter results; as such, cefoxitin might be a more appropriate indicator of multidrug resistance in these organisms.40 Alternative procedures, such as polymerase chain reaction, or latex agglutination have been used to detect the gene responsible for the formation of penicillin-binding protein 2a (mecA) of MRSA and other techniques such as pulse-field gel electrophoresis (PFGE) or multilocus sequence typing (MLST) that identify the specific strain of MRSA (eg. USA 100 or USA 300), It is likely that this area of diagnostics will be refined in the next decade. Antibiotics are associated with induction, selection, and propogation of MRSA. The wide use of cephalosporins, in particular, may have contributed significantly to the advent of MRSA. MRSA in human patients has evolved from a hospital-acquired (HA-MRSA; nosocomial), in which occurs most commonly in patients immunocompromised by disease, drugs, procedures and duration of hospitalization, to a community acquired infection (CA-MRSA), in which otherwise healthy persons are infected, usually in the skin or soft tissue. Crowded conditions, shared items and poor hygiene increase the risk of community acquired infection. Although it is community acquired MRSA strain USA300 that appears to be most commonly associated with increased colonization in dogs and cats, it is USA100, most commonly associated with hospital acquired-MRSA infections in humans, that most commonly is associated with infections in dogs and cats animals 302 According to the Center for Disease Control, the incidence of MRSA doubled in human medicine in the 7 year period between 1999 and 2006. The impact of MRSA in veterinary medicine is increasingly problematic, not only because of its impact on the patient, but the public health considerations. The mec gene has been detected in methicillin-resistant Staphylococcusaureus organisms infecting dogs40-42 and MRSA has been associated with infection in dogs.43 However, MRSA also has been found in up to 4% of healthy dogs, with identification complicated by the need for multiple sampling sites (nasal and rectal or perineal). Risk factors for the presence of MRSA in pets or working dogs (ie, detection or aid dogs), include contact with human hospitals (particularly if patients were licked or patients fed the dogs treats) and children.42 Infections have been isolated in family members and pets in the same household, but this is likely to reflect transmission from humans to the pet.40-42,44 It is likely that colonization is transient in animals. However, healthy pets have been demonstrated to be potential reservoirs for transmission of MRSA to healthy handlers and a potential health risk to immunocompromised patients (human and presumably other animals in the household). According to the AVMA, colonization by MRSA is suggested to be an occupational risk for veterinarians, although the frequency of infection associated with MRSA in veterinarians compared to other professions has not been documented. Methicillin resistant Staphyloccoccus intermedius (pseudointermedius)45 has a prevalence of 0.58% to 2% in healthy dogs and up to 4% healthy cats42,46 with the mec gene present in each canine MRSP isolate in one study.47 Human colonization with MRSP is unusual.42 However, MRSP has been reported as a cause of infection in human patients 42 and transmission from pets with pyoderma has been confirmed.48,49 Although the true public health significance of MRSA and MRSP (or other MDR ognaisms) in pets is not clear, the fear of infection may be as important as true risk, necessitating proper hygiene and other proactive measures such that human or animal health (including unnecessary euthanasia) are not risked. The American Association of Veterinary Medicine offers a website that includes a discussion of MRSA zoonoses, including sources of guidelines that might decrease the risk presented to susceptible humans (http://www.avma.org/reference/backgrounders/mrsa_bgnd.asp; accessed January 01, 2010). Among the more important actions that can be taken is establishment of infection control policies and guidelines in each veterinary practice. In general, commen sense approaches should prevail (eg, minimizing intimate contact, personal and environmental hygiene, etc). This includes cleansing of hands of handlers, and the paws (or body?) of animals that might be exposed to MRS, including those visiting human health care facilities. The risk of colonization is increased 6 fold in aid animals (those providing assisted interventions for humans). It is the very immunocompromised patient that is at risk for MRS infection acquired from an animal. In such cases, the carrier or infected animal should be removed from the environment until successfully treated for methicillin-resistant Staphylococcus. For dogs with skin infections, cultures are indicated to detect MRS, particularly in animals for which infection does not resolved. Successful resolution of colonized or infected animals may require both topical (for skin infections) and systemic therapy may be indicated. Evidence of successful treatment might be based on skin swabs of the ear, nose and perianal region. Care must be taken to assure that the laboratory providing culture procedures is well-versed in the diagnosis of MRS, including speciation of coagulase positive organisms. The multidrug resistance associated with MRSA is now evolving toward other (non-beta lactam) antibiotics. This reflects in part, other resistance genes in the gene cassette carrying the mec gene.42 Drugs that are impacted include fluorinated quinolones and aminoglycosides. Although newer fluorinated quionlones (e.g., levfloxacin) appear to be more effective than older drugs in vito, particularly to Staphylococcus, it is not clear if this translates to better clinical efficacy.21 Glycopeptides such as vancomycin are the initial drugs used to treat MRSA in humans, although increasingly vancomycin resistant staph infections (VRSA) have emerged. Multidrug resistant Enterococcus also is an emerging issue; its emergence also appears to be correlated to use of cephalosporins. Enterococcus faecalis more so than Enterococcus faeclis is likely to develop resistance and speciating Enterococcus on susceptibility testing might be prudent. Resistance reflects a change in PB-V and the risk is increased when drugs effective against Enterococcus are used. Detection of MRSA on C&S generally is based on resistance to oxacillin, which is more stable in disks used for testing. Over the 30 to 40 years since the methicillin resistant classification was coined, the infections associated with the organisms have lead to increasing mortality and morbidity. Susceptibility to a number of alternative antimicrobials, including fluorinated quinolones, aminoglycosides, and glycopeptides (vancomycin) is now decreasing.
The "Other" E. coli.
Escherichia coli, a member of the family Enterobacteriaceae, 9-10 is the predominant facultative anaerobe (in the normal intestine of both humans and many warm-blooded animals.1-2 Referred to as the "cockroach" of microbes because of its adaptability, E. coli rapidly divides, potentially doubling its population every 20 minutes. Further, it is highly mutagenic, with spontaneous mutations occuring in of 1 per 100 thousand to 1 per billion new progeny (assume 1 gm of feces contains 100 million E coli) thus assuring opportunity for spontaneous mutation even in the absence of stimuli, such as drugs. Virulence and resistance are characteristics of concern for the patient infected with this organism. Virulence refers to the ability of an organism to cause disease whereas resistance refers to the ability of the organism to avoid harm, although clinically we tend to use the term in reference to avoidance of harm caused by antimicrobials. Resistance and virulence are often perceived to emerge simultaneously. Recently, however, studies suggest that resistance may be associated with a reduced potential for invasiveness and a decrease in the presence or the expression of some virulence factors in E. coli.11-20
Virulence.
Although enteric E.coli are generally nonpathogenic, the presence of virulence factors in some strains3-4 allows classification of E. coli into 6 groups capable of causing enteric disease: Enteropathogenic E. coli (EPEC), Enterotoxigenic E. coli (ETEC), Enterohemorrhagic or Verotoxigenic E. coli (EHEC or VTEC), Enteroinvasive E. coli (EIEC), Enteroaggregative E. coli (EAggEC), Uropathogenic E. coli (UPEC) and diffusely adherent E. coli (DAEC).5-6 Extraintestinal E coli (ExPEC) is a more recently classified pathotype; UPEC are included in this category. Although much attention has focused on the impact of enteropathogenic E. coli (e.g., OH157:H7) in human medicine, other E. coli, particularly ExPEC, also are associated with morbidity and mortality.15,16 These include sepsis associated (SEPEC) and neonatal meningitis associated (NEMEC) E. coli. The ExPEC appear to easily colonize the gastrointestinal tract, potentially displacing commensals, and eventually emerging as infectious organisms in other body tissues, particularly in the urinary tract.17-20 Fecal E. coli from healthy dogs have been reported to poses virulence factors considered as markers of enteropathogenicity. Examples include eae and sta genes, heat-stable enterotoxin, verotoxin, iron uptake mechanisms (siderophores) which facilitate survival and replication, and hemolysin and cytotoxic necrotizing factor (cnf).6, 8-10 The latter two virulence factors are exotoxins capable of causing harm to eukaryotic cells. They facilitate extraintestinal infection as is exemplified by cnf and its influence on UPEC infection of the urinary tract . 9 Siqueira118 has reported a high frequency of virulence factors associated with E. coli isolated from dogs with UTI (n=51), pyometra (n=52) and feces of healthy dogs (n=55). These factors are of concern not only to the small animal clinician, but increasingly are contributing to a potential public health concern . Studies have demonstrated transfer of resistant E. coli between animals and humans, a fact which was documented as early as 197522 . Canine E. coli strains have been demonstrated to be phylogenetically similar to pathogenic strains infecting humans. Over 15% of environmental canine fecal deposits contain E. coli strains related to virulent human strains.23 Evidence that pets and owners share E. coli is increasing as has been demonstrated in studies within family members, including pets. 24-28
Resistance.
The gastrointestinal environment is conducive to development of resistance. Environmental microbes maintain an ecological niche by suppressing competition through secretion of antibiotics. As such, commensal organisms are constantly being exposed to antibiotics. However, the microbe producing the antibiotic, as well as surrounding normal flora, are resistant to the antibiotic. Thus, genes for resistance develop along with genes directing antibiotic production and organisms are "primed" to develop resistance. Microflora of the GI tract can serve as reservoir of resistance genes. Exposure to antimicrobials may facilitate survival of isolates that have either spontaneously mutated or acquired resistant through other means.21 Resistance may be easily conferred to other potentially more virulent organisms.22 E. coli rapidly develops resistance, particularly that associated with multiple drug resistance (MDR) when exposed to selected antimicrobials. More disconcerting, resistance is easily conferred to more pathogenic organisms. In human medicine, E. coli has developed resistance to the fluorinated quinolones, beta-lactams, or both ; it is among the Gram negative organisms that secrete extended spectrum beta-lactamases (ESBL). E coli resistance in isolates associated with urinary tract infections is particularly well described . One study demonstrated the gastrointestinal emergence of quinolone -resistant E. coli genetically distinct from infection-causing strains in patients treated with ciprofloxacin.Like virulence factors, transfer of resistance genes in isolates between animals in humans may present a public health risk, as was recognized by the FDA by 1999. E. coli develops resistance both vertically and horizontally. Shared resistance reflects the ability of bacteria to incorporate extrachromosomal DNA carrying the information for resistance from other (including non-self) organisms. Extrachromosomal DNA (including plasmids and bacteriophages) encode for resistance to multiple drugs and can be transmitted vertically (to progeny) or horizontally, across species and genera. Transposons are individual or clusters of resistance genes or repeated DNA sequences (two conserved DNA segments on either side of a resistant gene. Transposons move resistance genes back and forth between chromosomes to plasmids. Integrons are able to capture genes encoding antimicrobial resistance and, unlike transposons, code for an integrase gene. The genes for resistance are located on a gene cassette that can exist as free, circular DNA, but unlike plasmids, can not be replicated or transcribed. Ultimately, the integron must re-integrate into bacterial DNA. As such, bacterial resistance is extremely mobile, and can spread rapidly. In general, resistance carried by plasmids "comes and goes", meaning the presence of the drug may increase the likelihood of the plasmid being present, in large copy numbers; removal of the drug may be associated with resolution of the resistance.

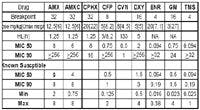
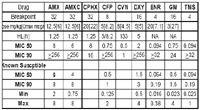
The MIC 50 and 90 for E. coli collected from dogs or cats. To use this chart for dosing, use the top set of data if the susceptibility status of the isolate is not known (for cephalothinand cefovecin, the data is relevant only for animals not previously receiving antimicrobials; for isolates known to be susceptible, use the bottom set of data. The MIC 90 should be considered "what is needed" and the Cmax "what is achieved". For concentration dependent drugs (ENR and GM), the Cmax:MICshould be > 10. For the remaining drugs, which are time dependent, begin with the Cmax and for each half-life, decrease it by 50%. When the Cmax reaches the MIC 90, this represents T>MIC. Dividing the T>MIC by 0.5 to 0.75 (preferred) indicates the interval that the drug should be adminsitered.
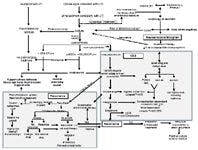
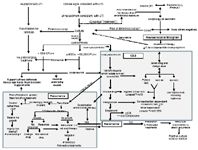
Rapid microbial turnover in the gastrointestinal tract supports the development of E coli vertical resistance (genomic change that is transmitted to offspring). Chromosomal (DNA) mutations are DNA mistakes that have been missed by bacterial repair mechanisms and occur at a rate of 1 per 107 to 1014 cell divisions. These mistakes occur spontaneously and randomly, resulting in resistance to a variety of compounds, including drugs, whether or not any antibiotic is present. Every time an antibiotic is administered, the normal flora is exposed to varying concentrations of the drug. If the mutation that confers resistance occurs in the presence of the antibiotic, the surviving mutant can progress to a single step mutation, conferring a low level of resistance. The surviving mutants divide, reaching a large enough population to cause infection, with the MIC of the second infection likely to higher than the first. Spontaneous mutations continue, and further microbial turnover can lead to multi-step mutations and rapid emergence of high-level resistance (eg, unlimited regulation of beta lactamase production, initiation of efflux pumps) characterized by increasingly higher MIC. Stepwise mutations can lead to specific resistance (ie, to a single drug or drug class), exemplified by clinical resistance to fluorinated quinolones which reflects stepwise mutation in DNA gyrase. Indeed, the most common mechanism by which E. coli develops resistance to fluoroquinolones reflects a point mutation in its topoisomerases, precluding binding of the drug to the protein. However, substitutions within the topoisomerase genes is also accompanied be an decrease in the outer membrane porins and overexpression of multidrug efflux pumps. Several classes of efflux pumps are active in E coli. The most important belongs to the RND family and is referred to AcrAB-TolC.47, 50-52 This pump system is associated with broad substrate specificity and thus serves to efflux many drugs from the bacteria, contributing to multi drug resistance.
The author has demonstrated the role that antimicrobial use has in contributing to E. coli resistance. Using the E-test® (for its wide range of drug concentrations) and standard veterinary antibiogram (to detect MDR), resistance in fecal E. coli was documented in normal purpose-bred dogs (3 per drug; 2 controls) after 7 days of dosing with either amoxicillin (10 mg/kg every 12 hr; top left) or enrofloxacin (5 mg/kg every 24 hr; middle left). For either drug, high-level resistance to that drug occurred by day 5 in essentially 100% of isolates. Total fecal coliform counts did not differ across time. For amoxicillin-treated dogs, E. coli resistance was directed only toward amoxicillin and steadily declined after the drug was discontinued, returning close to baseline by 3 weeks. For enrofloxacin-treated dogs, resistance was MDR and did not decline during the 21 post-treatment period.7, 51
Infection. Pathophysiology: Because it is normal flora, determining whether or not a cultured E coli isolate is pathogenic, that is, capable of causing host damage can be difficult.21 Yet doing so is prudent; indiscriminant use of antimicrobials contributes to the advent of resistance, as does in appropriate dosing regimens. Infection usually can be discriminated from colonization by the presence of large numbers of organisms, particularly if the culture is pure. Infection also is indicated by the presence of inflammation and phagocytized bacteria. E. coli is one of the more common pathogens infecting many tissues. One study of 674 E. coli isolates collected from dogs found the far majority (n=424) associated with urinary tract infections (UTI) however, 61 were also collected from skin, respiratory tract (52), ear (43), female (42) and male (25) reproductive tracts, and (23) other organ systems. In dogs, a variety of E. coli strains including attaching and effacing E. coli (AEEC), necrotoxigenic E. coli (NTEC), ETEC and VTEC have been associated with diarrheal diseases.7 Strains causing pyometra in dogs have been demonstrated to be similar to those causing UTI. 118
The role of Escherichia coli as a cause of UTI is well known, being recognized as the predominant cause of UTIs in both dogs and cats.107,108 A number of reports have confirmed E. coli as the predominating organisms causing UTI, particularly in dogs, but potentially second to Enterococcus in cats. Ling105 found that most UTI were caused by a single agent, with E. coli the organism most commonly isolated (45%, Table 10.1). A retrospective study of UTI in dogs admitted to a veterinary teaching hospital and subsequently diagnosed with UTI (n=240);112 found E. coli was the causative organism in 50% of the cases, with the majority of the remaining organisms being Gram negative coliforms (e.g., Proteus, Klebsiella). E. coli also is a common cause of recurrent UTI. Sequin retrospectively examined recurrent UTI in dogs (n=441 isolates from 373 positive cultures). E. coli (47%) was the most commonly isolated, followed by Enterococcus (21%). The identity of the UPEC as a common infecting organism of UTI reflects its pathophysiology . Ascending infection from the urethra is by far the most common route of infection in UTI. In both humans and dogs, the origin of bacteria infecting the urinary tract is generally fecal, with The frequency of infection by a particular strain depending on the virulence of the organism. Pathogens generally travel along the urethra to the bladder. Anatomic deformity and turbulent urine flow may facilitate antegrade movement of organisms toward the bladder. Female patients are more predisposed to ascending infection due to the shorter length of the tract and increased risk of contamination. Once in the bladder, infection can continue to ascend up the ureter to the kidney, particularly if vesiculoureteral refux is present. Uropathogenic E coli (UPEC) are capable of causing extraintestinal infection because they contain specialized virulence factors and as such, differ from commensals. Escherichia coli contains adhesins that bind to the glycolipid receptors. Mannose-containing receptors also have been documented in humans; E. coli (and other Enterobacteraicea) carries mannose-specific adhesions which, upon entry into the lower urinary tract, appear to be the primary mechanism of adherence for E. coli and thus are important for colonization of the bladder or lower structures. In contrast, mannose-resistant fimbriae and other adhesins appear to be critical for colonization of the renal structures. Binding between receptor and adhesin changes the receptor-bearing cell. The severity of a UTI may be correlated with the degree of adherence to uroepithelial cells. Organisms causing acute pyelonephritis in human patients are characterized by higher adherence compared with organisms causing asymptomatic bacteria. These E. coli produce a number of virulent factors, including hemolysin and aerobactin, and are able to resist the antibacterial effects of serum.117 Toxins such as endotoxin may act in conjunction with adherence to induce inflammation. Eventually, identification of virulence factors may facilitate detection of infection in tissues other than the uroepithelium, providing guidance regarding treatment. The Three "DE"s. The most significant mechanism by which bacterial resistance is likely to be reduced is implementation of behaviors that are designed to reduce patient risk such as length of hospital stay, and design, implementation of and adherence to infection control practices.. Consider the three DEs: (1) DE-ESCALATE. Because previous antimicrobial therapy is one of the most important factors associated with resistance, approaches which minimize indiscriminant antimicrobial use will be important. Examples of human strategies include improving appropriate antimicrobial use (eg, including less ideal strategies such as strict adherence to prescribed formularies, setting limits on the duration of antimicrobial therapy); potentially reasonable strategies such as requiring prior approval for use of certain antibiotics such that proper use can be verified; and more rationale strategies such as narrowing the spectrum of empiric antibiotics, and rotating the use of antimicrobial drugs on a regular schedule); primary prevention by decreasing length of hospital stay, decreased use of invasive devices, and newer approaches such as selective digestive decontamination and vaccine development. Probably the single most important first step in judicious antimicrobial use and avoiding resistance is questioning/confirming the need for therapy. This is no small task, being frought with the lack of effective diagnostic aids. Probably the most common– and least correct mindset is failure to recognize that we are in conflict with our directive of "above all else do no harm" if we use antimicrobials in the absence of infection. De-escalation includes taking actions that stay the hand in reaching for drugs if they are not really necessary. The second De is (2) DESIGN. Dosing regimens should be designed to assure that adequate drug concentrations are reached at the site of infection to kill, not simply inhibit, microbial growth. DEAD BUGS DON'T MUTATE! Once the decision to use the antimicrobial is made, efforts should focus on assuring that concentrations adequate to kill the infecting microbe are achieved at the site of infection. The final De is (3) DETERGENT: Hospital strategies include: improving infection control (eg, selective decontamination procedures, prevention of horizontal transmission via handwashing, use of disinfectants, glove and gown use, alternatives to soap, and improving the workload and facilities for health care workers), and identification of specific areas for treatment of potentially infectious agents (ie, bandaging areas that can be easily cleaned). Increasingly "detergent" should be applied to the patient and its home. For example, recurrent infections might be reduced if successful initial therapy is coupled with cleansing of the environment in which the pet is located such that it is not continued to be exposed to the infecting bug.
Facilities for health care workers), and identification of specific areas for treatment of potentially infectious agents (ie, bandaging areas that can be easily cleaned). Increasingly "detergent" should be applied to the patient and its home. For example, recurrent infections might be reduced if successful initial therapy is coupled with cleansing of the environment in which the pet is located such that it is not continued to be exposed to the infecting bug.
No portion of this manuscript may be reproduced without author consent. References limited by request.