Diagnosing forelimb lameness in dogs (Proceedings)
Osteochondritis dissecans OCD is a manifestation of osteochondrosis in which a flap of cartilage is lifted from the articular surface.
Osteochondritis dissecans (OCD) is a manifestation of osteochondrosis in which a flap of cartilage is lifted from the articular surface. Osteochondrosis is thought to proceed OCD and is a disturbance in endochondral ossification. The disturbance in endochondral ossification leads to multiple areas of cartilage islands on the surface and within the humeral epiphysis which have not undergone normal maturation into bone.
Areas of abnormal endochondral ossification of the articular surface become thickened and are susceptible to fissure and loosening (OCD) as the deeper chondrocytes undergo necrosis due to inadequate nutrition and a suboptimal microenvironment.
Large and giant?breed dogs are commonly affected and males are more often affected than females. Clinical signs often develop between 4 and 8 months of age; however, some dogs may not be presented for veterinary evaluation until they are mature. Affected animals are usually presented for examination because of unilateral forelimb lameness. Owners usually report a gradual onset of lameness that improves after rest and worsens after exercise.
On physical examination, the shoulder should be palpated and moved through a complete range of motion. Crepitation or palpable swelling of the joint is seldom evident, but affected animals usually exhibit pain when the shoulder is moved into hyper-extension or extreme flexion. Often the examiner can detect muscle atrophy of the forelimb by loss of muscle mass adjacent to the spine of the scapula.



Radiographs
Despite apparent lameness in only one limb, both shoulders should be radiographed because this condition is often bilateral. Sedation may be required for quality radiographs particularly in large hyper-active dogs. The earliest radiographic sign of OCD is flattening of the caudal humeral head. This is due to thickening of the articular cartilage and deviation of the subchondral bone line.
As the disease progresses, a saucer?shaped radiolucent area in the caudal humeral head may be visualized. Calcification of the flap may allow visualization of the flap either in situ or within the joint if it has detached from the underlying bone. In chronic cases, large calcified joint mice are often observed in the caudoventral joint pouch or cranially within the bicipital groove.
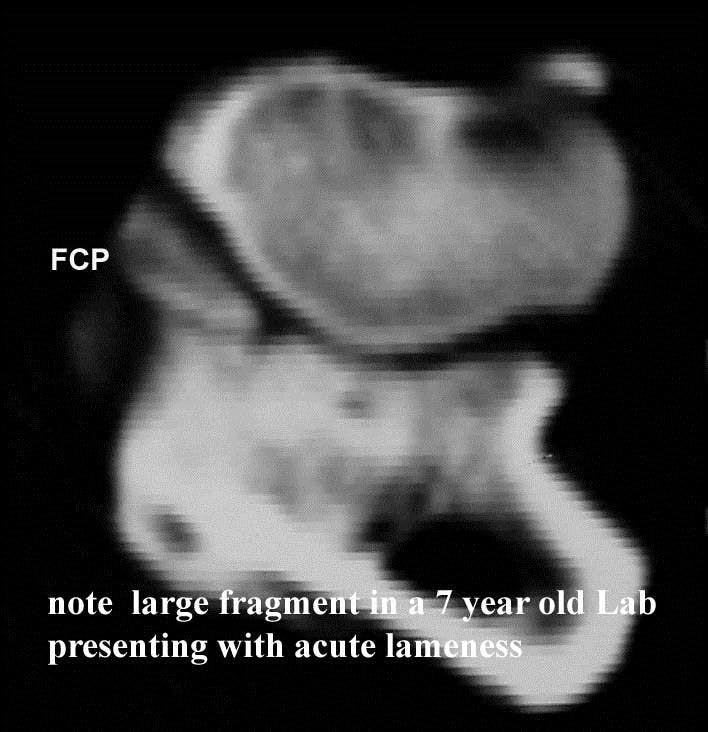
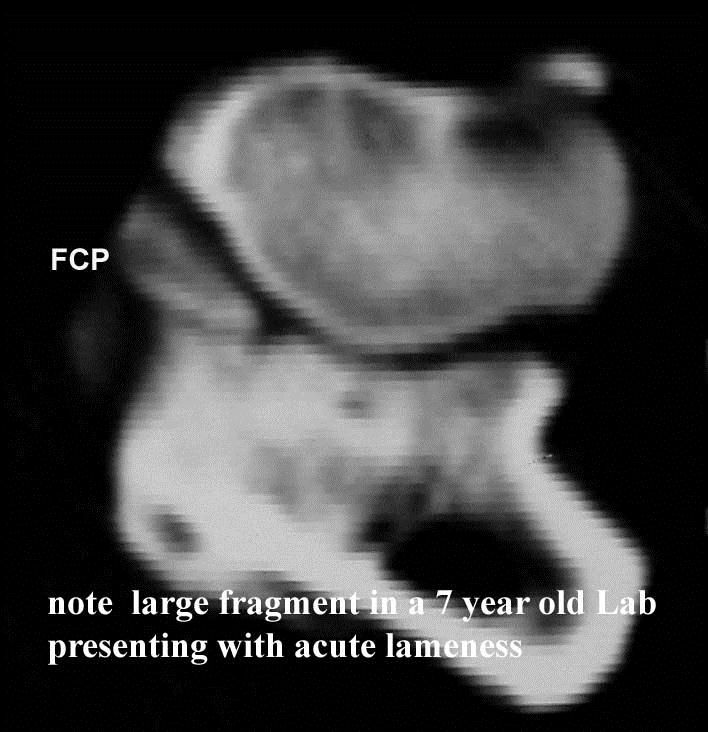
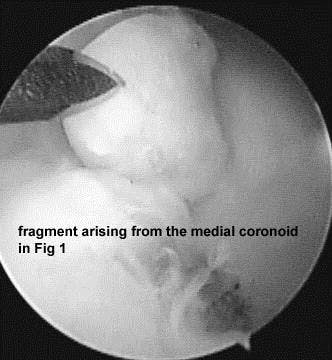
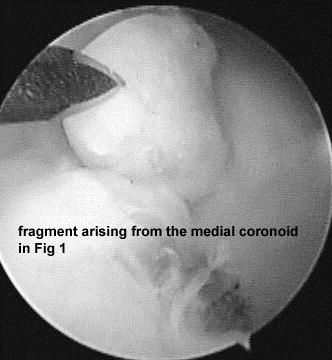
Forelimb lameness can be a diagnostic challenge in the athletic dog; often the lameness has been treated for months with no improvement. The only abnormal physical finding may be the observation of Grade 2 or Grade 3 lameness. The source of lameness may be attributed to soft tissue injury, bony injury or a combination of both. In the active adult dog the most common cause of latent forelimb lameness can be attributed to pathology in the elbow and to injury of the active and passive shoulder restraints. In the author's experience, pathology in the elbow is regularly caused by occult microfracture/fragmentation of the medial coronoid process. There is no joint effusion, loss of motion, pain, or crepitus on physical examination. Radiographs are reported as normal or may show minimal subtrochlear sclerosis of the ulna.
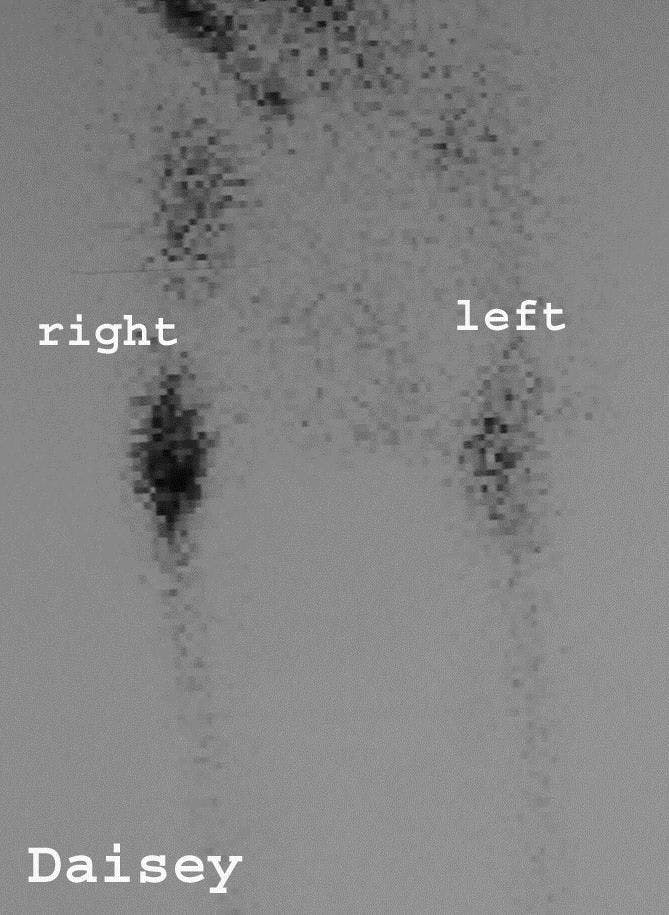
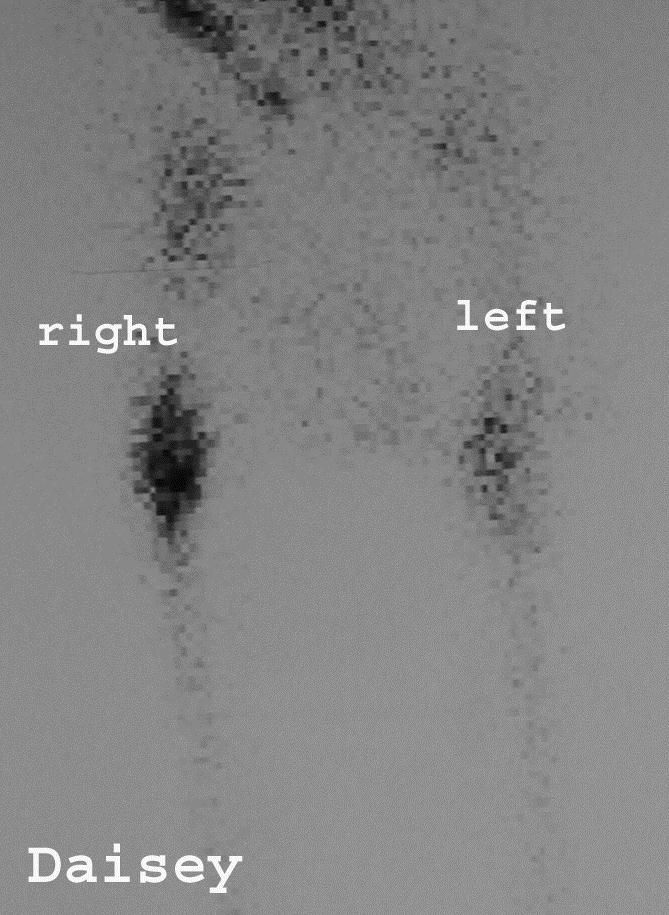
Figure 1






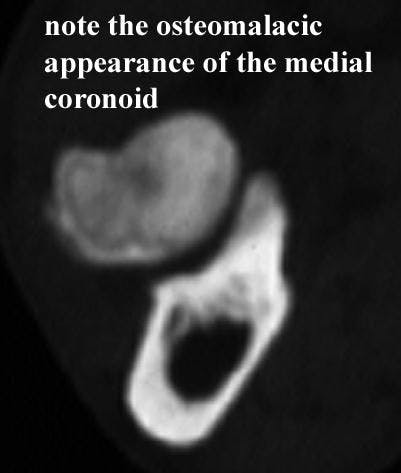
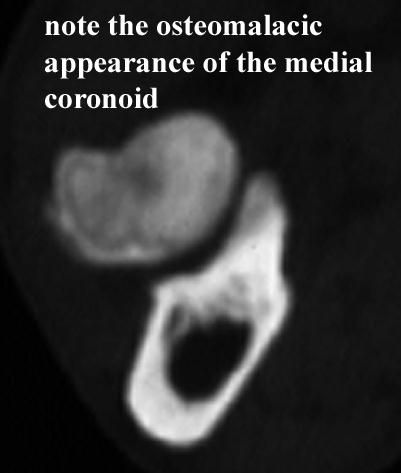
Modalities to facilitate an accurate diagnosis in these cases are CT, nuclear scan, and arthroscopy. Recommendations for performing CT include scanning from the point of the olecranon to 2cm distal to the radial head. Scan thickness should be 1-2mm with .5mm overlapping slice index. Transverse slices using 1500 to 3500 HU are ideal for imaging subchondral bone and fragments of the medial coronoid; transverse images at 3500HU are considered ideal for identifying ostomalacic lesions of the medial coronoid.


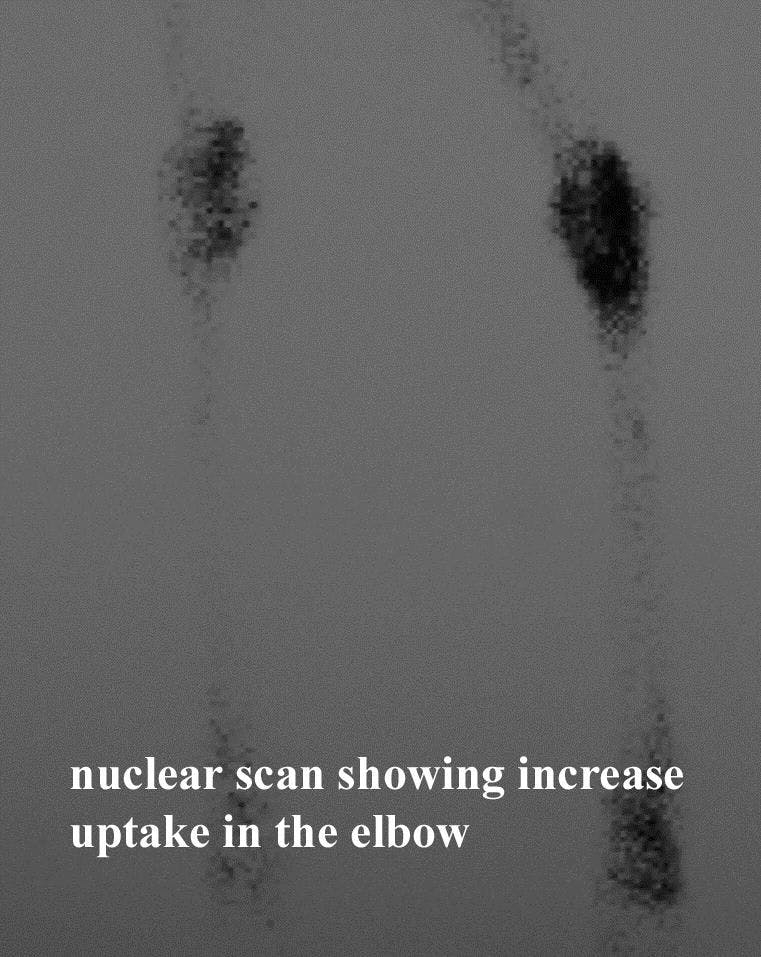
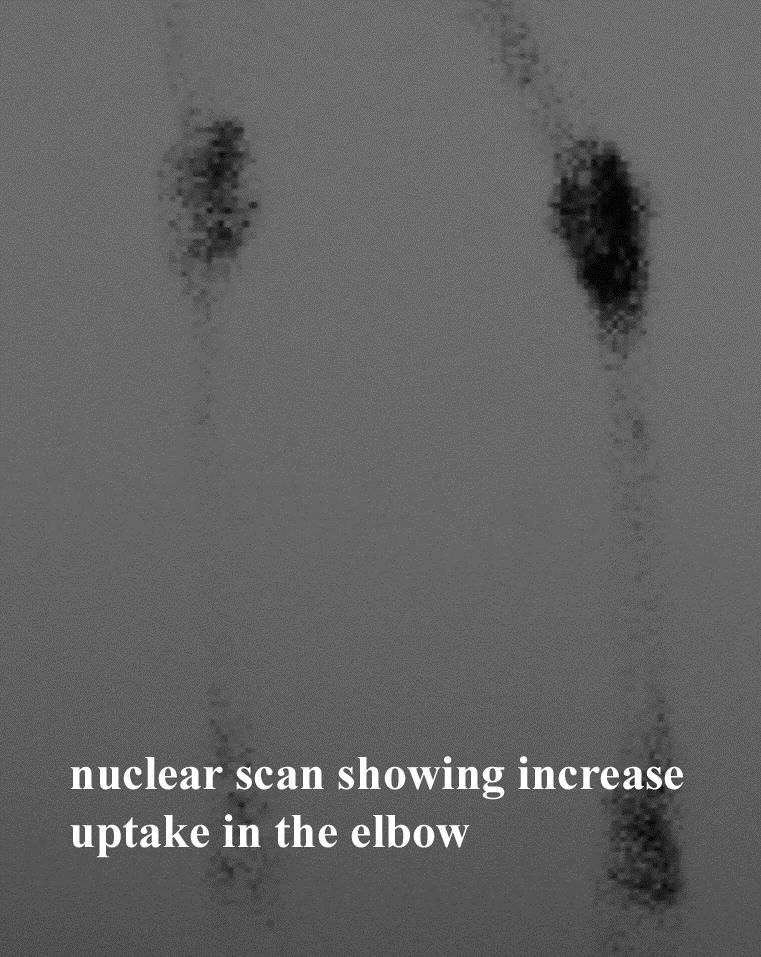
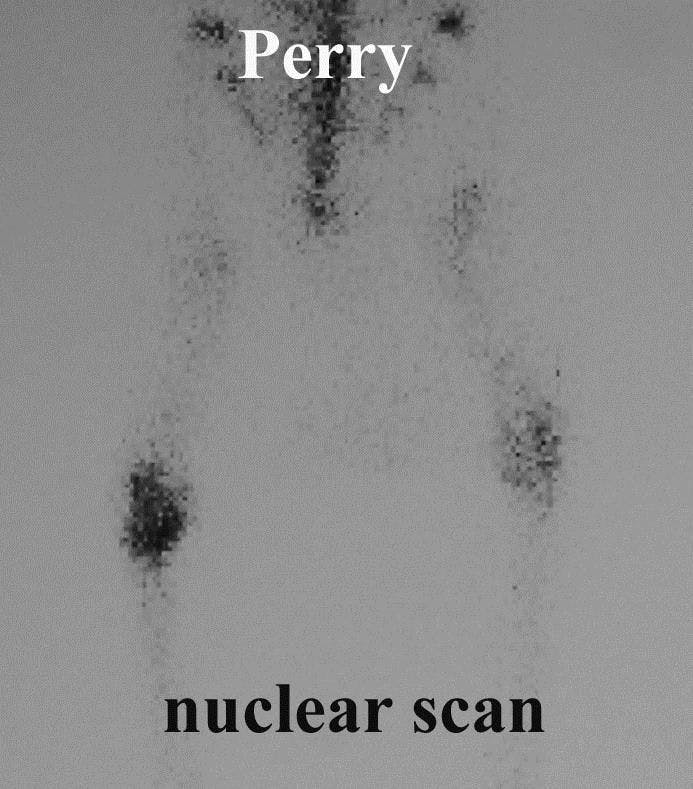
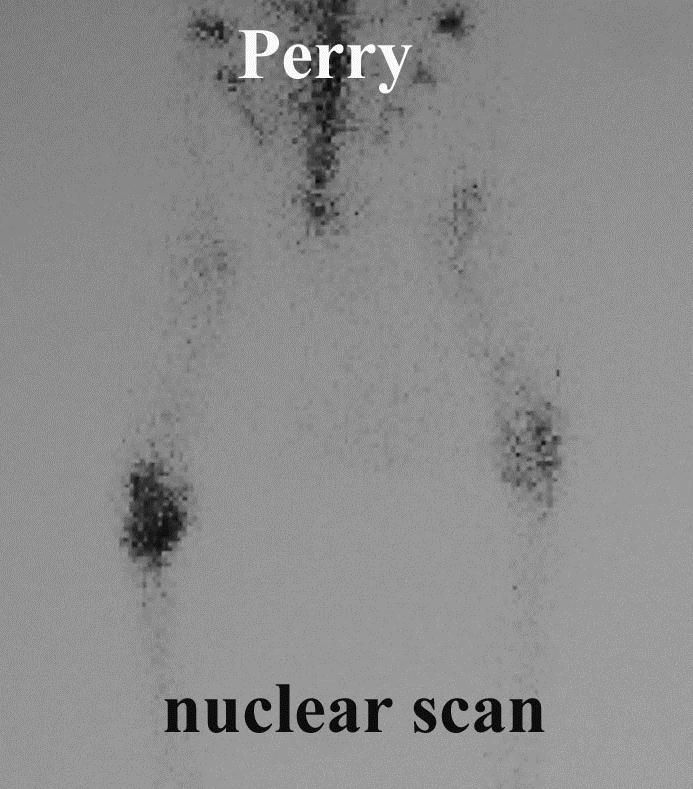
Nuclear scintigraphy can be used to localize the origin of the lameness and can be used to facilitate detection of subtle pathologic changes before changes are evident of radiographs. Technetium phosphonates are typically used for scintigraphy of joint tissues. Scintigraphy has high sensitivity for detection of presence of elbow pathology but is not specific for definitive diagnosis. Regulatory issues often limit the use of scintigraphy to academic institutions or large referral practices. Nevertheless it is invaluable facilitating lesion localization in dogs with forelimb lameness. Most commonly, it is used to rule in or rule out elbow pathology. Note in the cases shown below the uptake in technetium in the involved elbow compared to the normal elbow. Each of the below cases had a long standing undiagnosed forelimb lameness. Radiographs of these cases were considered within normal limits. The use of scintigraphy localized the lesion to the elbow which then allowed application of more specific diagnostic modalities such as CT or arthroscopy.



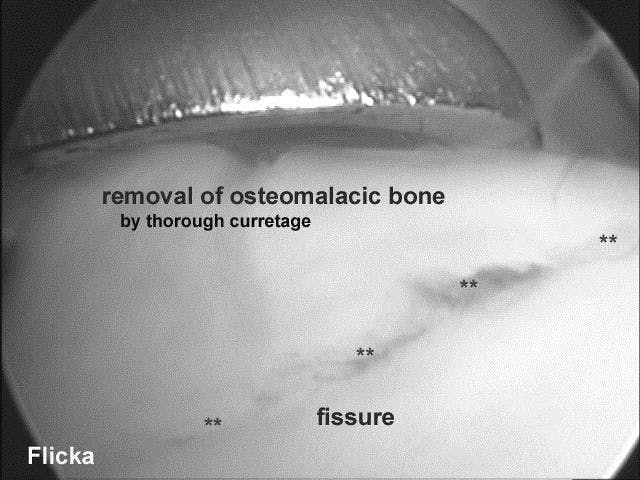
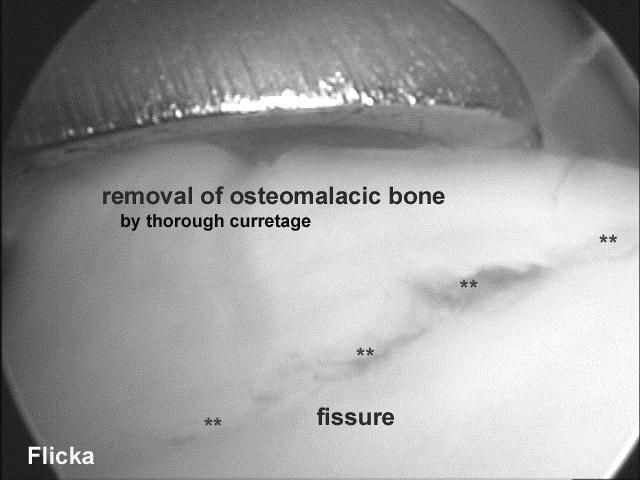
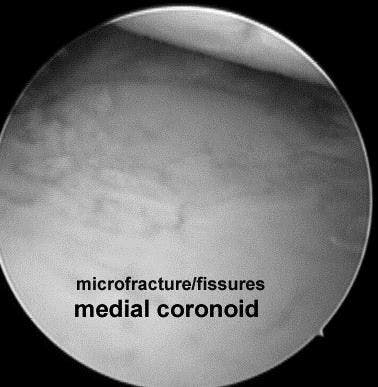
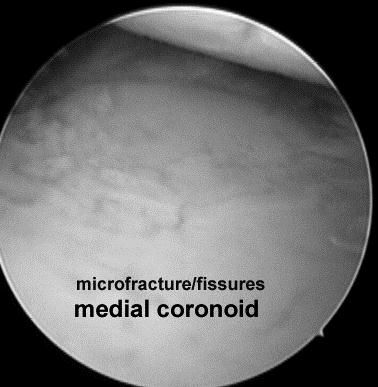
Arthroscopy is more invasive than imaging modalities but is very specific for identification of pathology in the medial compartment of the elbow. A comparison of CT with arthroscopy showed that these procedures were complimentary for medial coronoid assessment. Care must be exercised when assessing the medial coronoid on CT and arthroscopically. Fragmentation of the articular cartilage, micro fissures and nondisplaced fragments may not be detected on CT. Likewise, with arthroscopy, thorough probing and or curettage adjacent to the radial head often will reveal abnormal bone or fragments beneath the cartilage surface not visualized on with casual observation.



Active and passive restraints of the Shoulder: Diagnosis and treatment
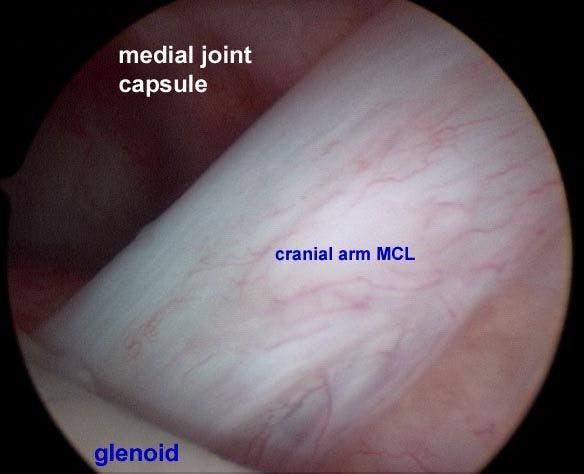
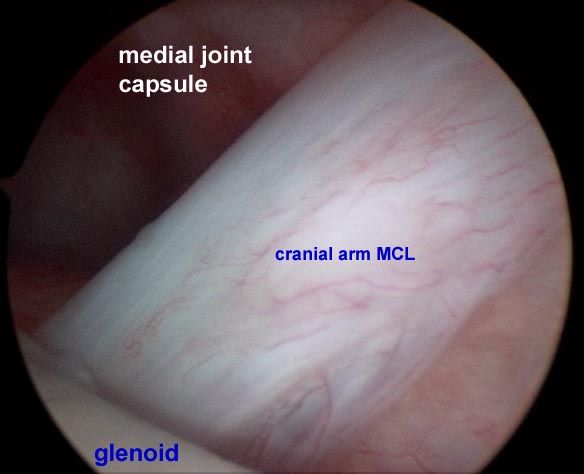
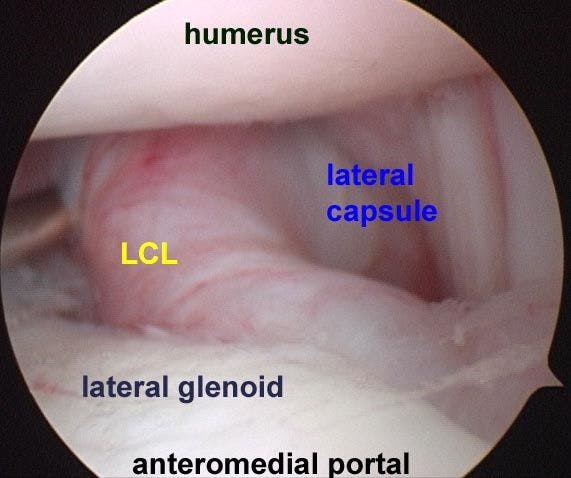
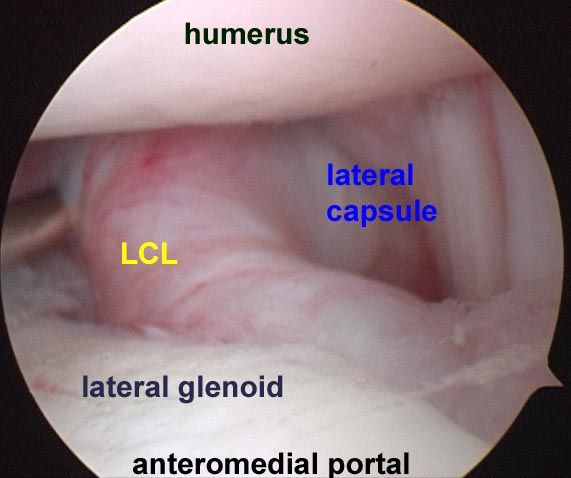
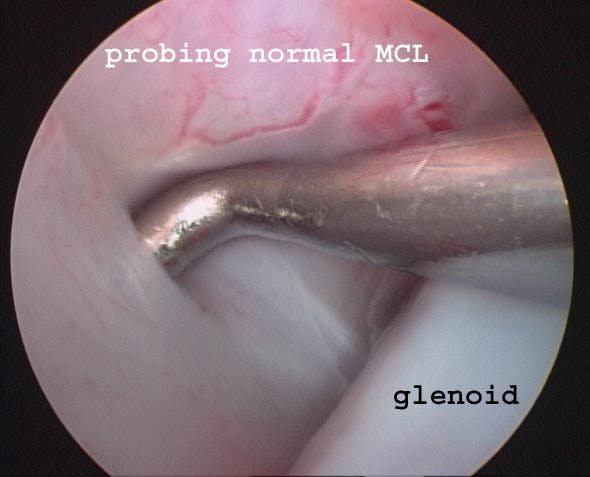
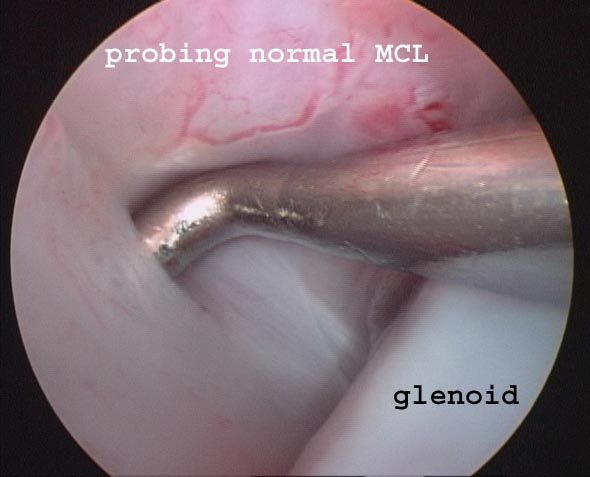
Forelimb lameness attributed to shoulder instability is reported frequently in the literature. Some orthopedic centers report the presence of subtle shoulder instability frequently where as others rarely diagnose the condition. The widespread difference in the frequency of diagnosis between clinics has led to disagreement relative to criteria for diagnosis of shoulder instability and the arthroscopic appearance normal intra-articular structures versus pathologic lesions. Stability of the shoulder is derived from passive and active restraints. Passive mechanisms include the medial and lateral glenohumeral ligaments, surrounding joint capsule, joint conformation, and synovial fluid cohesion. The medial collateral ligament (MCL) commonly appears as “y” shaped with the cranial arm coursing caudally from its origin at the medial surface of the supraglenoid tubercle. The caudal arm of the MCL originates from the medial surface of the scapular neck and joins the cranial arm to insert onto the humeral neck. The MCL and associated joint capsule is a major factor in providing joint stability; complete medial luxation occurs following transection of the MGHL. The lateral collateral ligament (LCL) originates from the lateral rim of the glenoid and extends ventrally to insert onto the humerus at the caudal region of the greater tubercle. The joint capsule originates from the periphery of the glenoid cavity. Medially, the joint capsule forms a synovial recess due to its attachment several millimeters proximal to the glenoid rim.


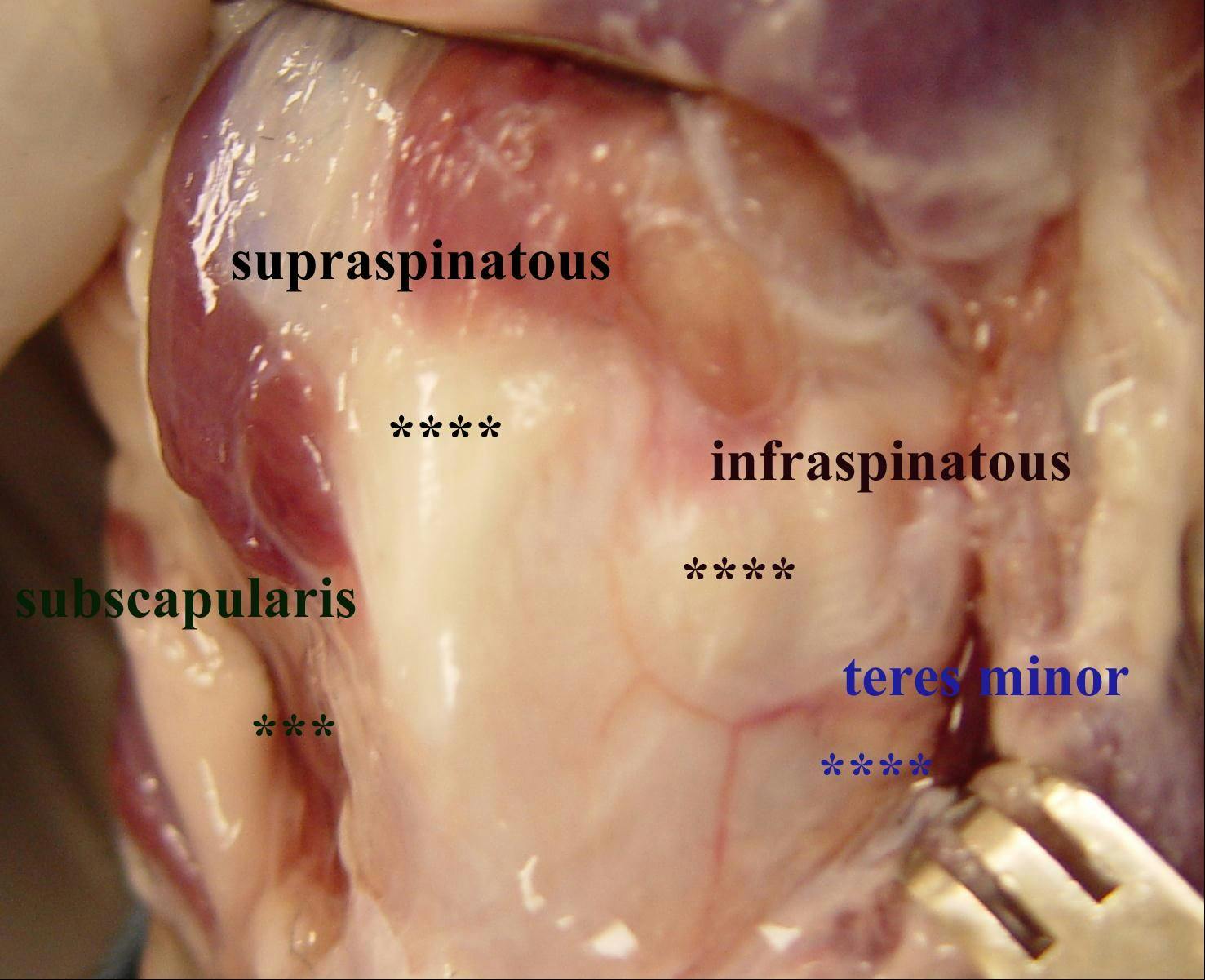
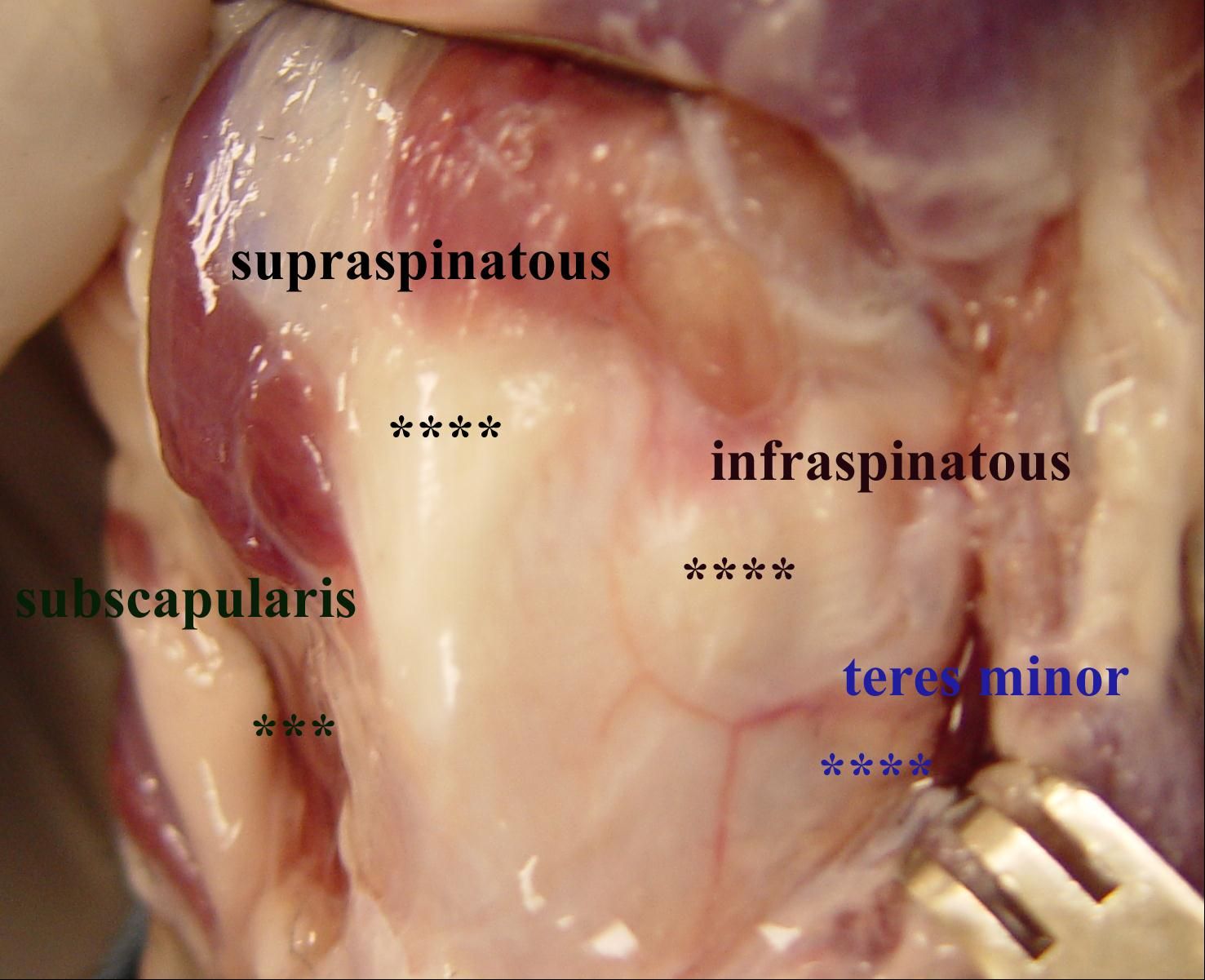
Dynamic active glenohumeral stability is provided by contraction of the surrounding cuff muscles. These include the biceps brachii, subscapularis, teres minor, supraspinatous, and infraspinatous muscles. Active contraction of all or selective cuff muscles induce compression across the shoulder joint as well as increasing tension in the joint capsule. When tested in neutral position, the cranial, lateral, and medial translation of the humerus was significantly increased after biceps tendon transection. In the flexed position, translation of the humerus in the cranial and lateral directions was significantly increased after biceps tendon transection. In the extended position, the medial translation of the humerus was significantly increased after biceps tendon transaction.


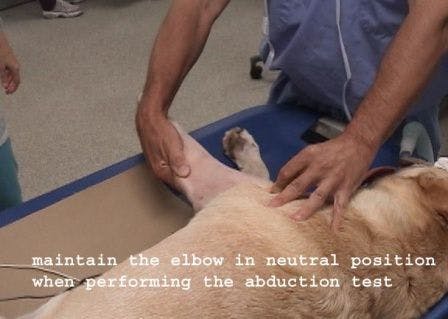
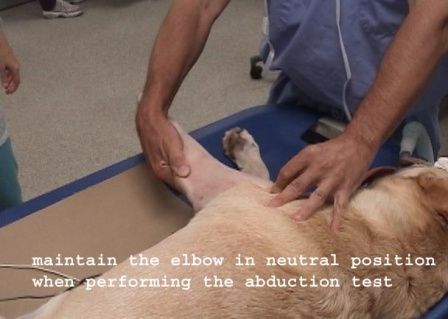
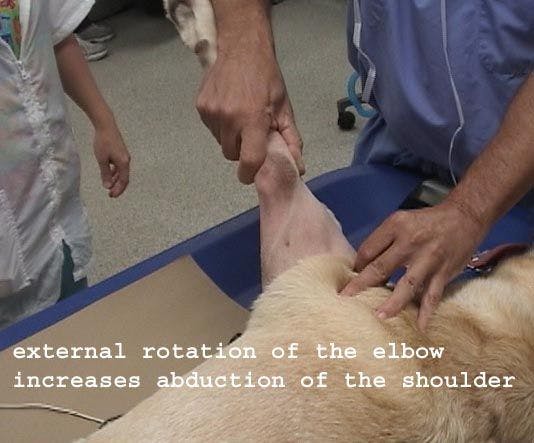
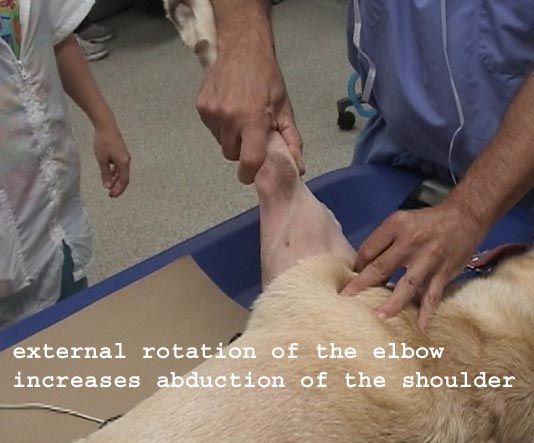
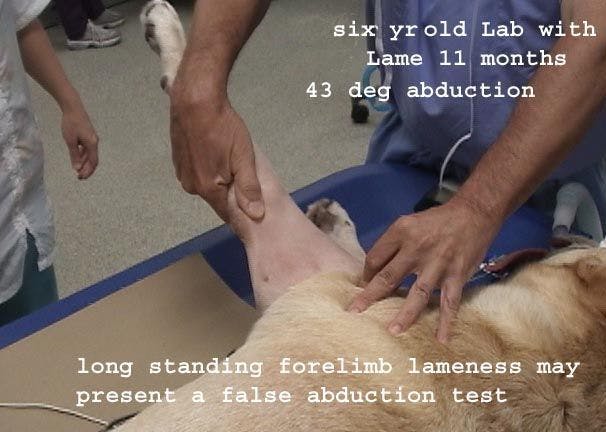
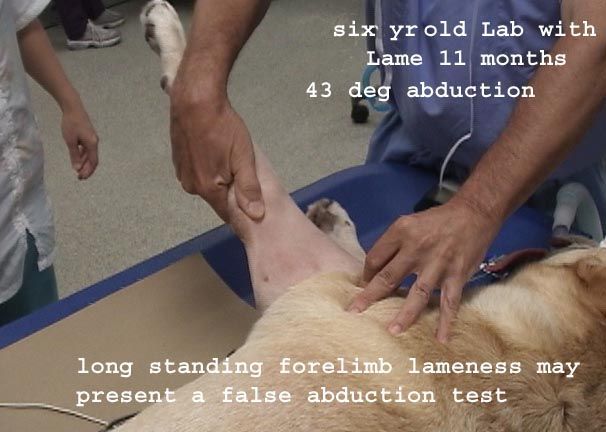
Examination of the shoulder for stability should be done under anesthesia or heavy sedation. Flexion, extension, abduction, craniocaudal translation, and rotational stability of the shoulder joint should be assessed. Normal range of flexion and extension are 40 degrees for flexion and 165 degrees for extension. Circumduction of the shoulder should not give rise to subluxation. Anteroposterior translation should be similar in both shoulders. A normal abduction test is approximately 23 degrees; abnormal abduction is considered present when abduction exceeds this degree and there is a difference in abduction angle between the injured side and the normal side. When performing the abduction test, it is essential to maintain the limb in extension with the elbow in neutral position, ie, one does not want the elbow externally rotated. If the elbow is externally rotated with the limb in extension, the shoulder joint will be internally rotated. The latter will give a false positive abduction test. To maintain the elbow in neutral position, the examiner should place his/her thumb on the lateral surface of the olecranon just posterior to the humeral epicondyle. Maintaining the thumb facing upward assures that the elbow remains in neutral position.


Care should be exercised in interpretation of side to side laxity difference. We have documented consistent abnormal abduction and AP translation is cases of long standing unilateral forelimb lameness. Our interpretation of shoulder laxity in these cases is that muscle and ligamentous atrophy give rise to increased shoulder laxity. In some cases, the shoulder laxity is secondary to long standing shoulder pathology such as OCD. Other cases are referred to our centers for treatment of shoulder pain. The pain is noted when the shoulder is placed in extension. By and large these cases are latent elbow dysplasia; the pain in fact arises from extension of the elbow when the shoulder is placed in extension.


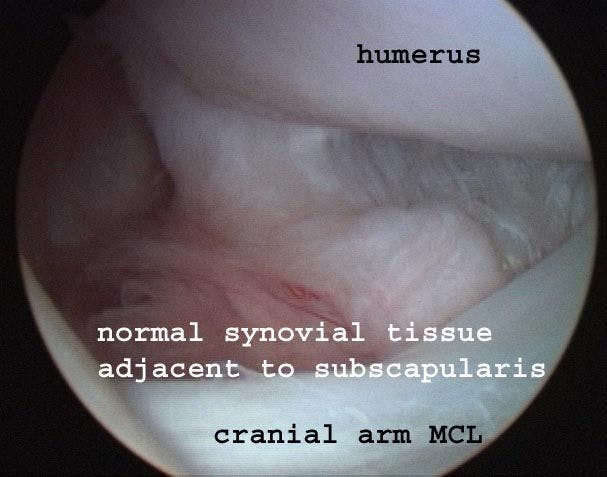
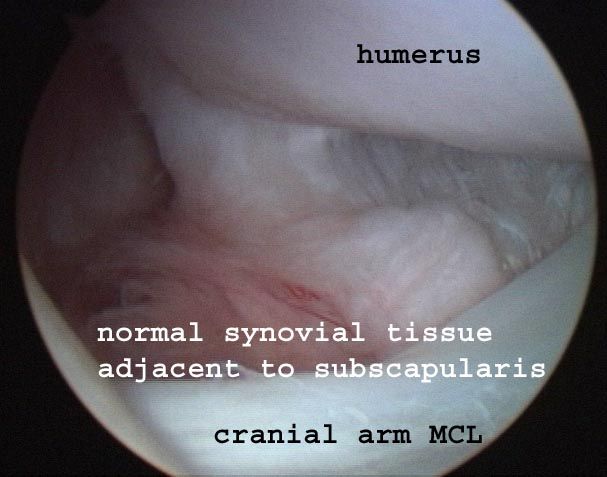
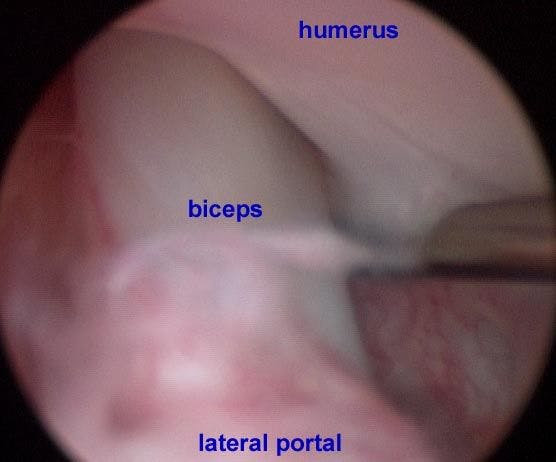
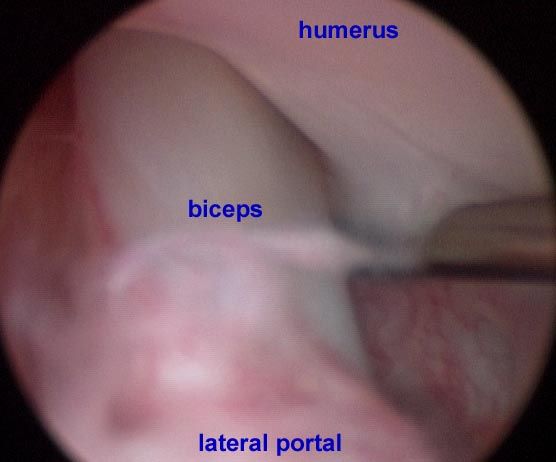
Debate continues amongst surgeons as to the interpretation of the arthroscopic appearance of intra-articular structures. Some surgeons believe it is possible to detect increased intra-articular volume and redundant capsular/ligament structures within the joint while others believe this cannot be accurately detected arthroscopically. Further, the significance of intra-articular lesions remains controversial. While some surgeons believe small tears of the cranial arm of the MCL result in instability and require treatment, others believe these small tears are insignificant and most likely iatrogenic. The gutter medial to the cranial arm of the MCL adjacent to the insertion of the subscapularis is often diagnosed as a site of trauma. However, this zone often shows synovial proliferation with pathologic conditions of the shoulder such as OCD.







 in general practice")






